Epidemiology Program, University of Hawaii Cancer Center, Honolulu, HI.
Office of Public Health Studies, University of Hawaii, Honolulu, HI.
Int J Cancer. 2018 Jul 15;143(2):263-268. doi: 10.1002/ijc.31311. Epub 2018 Feb 25.
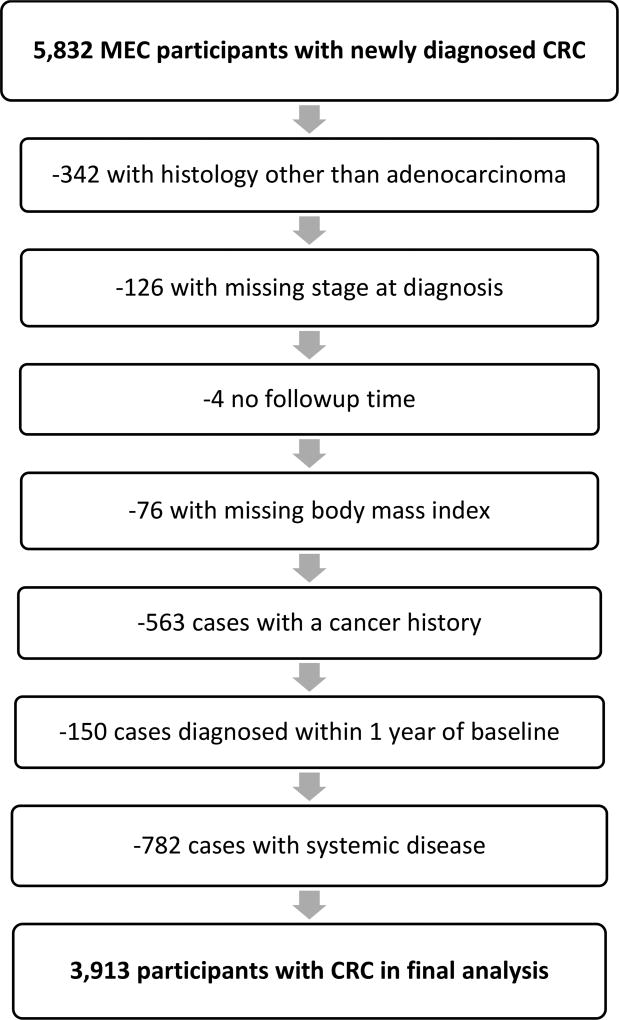
This analysis examined type 2 diabetes (T2D) as a predictor of colorectal cancer (CRC) survival within the Multiethnic Cohort Study. Registry linkages in Hawaii and California identified 5,284 incident CRC cases. After exclusion of cases with pre-existing cancer diagnosis within 1 year and systemic disease, the analytic dataset had 3,913 cases with 1,800 all-cause and 678 CRC-specific deaths after a mean follow-up of 9.3 ± 5.2 years. Among CRC cases, 707 were diagnosed with T2D 8.9 ± 5.3 years before CRC. Cox regression with age as time metric was applied to estimate hazard ratios (HR) and 95% confidence intervals (CI) for T2D status as predictor of CRC-specific and all-cause survival while adjusting for known confounders. Overall, CRC-specific survival was not associated with pre-existing T2D (HR = 0.84; 95% CI = 0.67-1.07). However, a significant interaction was seen for comorbidity (p = 0.03) with better survival among those without pre-existing conditions (HR = 0.49; 95% CI = 0.25-0.96) while no association was seen in patients with comorbid conditions. All-cause mortality was also not related to pre-existing T2D (HR = 1.11; 95% CI = 0.98-1.27), but significantly elevated for individuals with T2D reporting comorbid conditions (HR = 1.36; 95% CI = 1.19-1.56). Stratification by T2D duration suggested higher CRC-specific and all-cause mortality among participants with a T2D history of ≥10 than <10 years. The findings were consistent across sex and ethnic subgroups. In contrast to previous reports, pre-existing T2D had no influence on disease-specific and all-cause survival among CRC patients. Only participants with additional comorbidity and possibly those with long T2D duration experienced higher mortality related to T2D.
本分析考察了 2 型糖尿病(T2D)作为多民族队列研究中结直肠癌(CRC)生存的预测因素。在夏威夷和加利福尼亚的登记处建立了联系,确定了 5284 例 CRC 新发病例。在排除了 1 年内有预先存在的癌症诊断和系统性疾病的病例后,分析数据集有 3913 例病例,平均随访 9.3±5.2 年后有 1800 例全因和 678 例 CRC 特异性死亡。在 CRC 病例中,707 例在 CRC 诊断前 8.9±5.3 年被诊断为 T2D。应用年龄作为时间指标的 Cox 回归来估计 T2D 状态作为 CRC 特异性和全因生存的预测因素的风险比(HR)和 95%置信区间(CI),同时调整了已知的混杂因素。总体而言,CRC 特异性生存与预先存在的 T2D 无关(HR=0.84;95%CI=0.67-1.07)。然而,在共存疾病方面存在显著的交互作用(p=0.03),在没有预先存在的情况下生存更好(HR=0.49;95%CI=0.25-0.96),而在患有共存疾病的患者中没有关联。全因死亡率也与预先存在的 T2D 无关(HR=1.11;95%CI=0.98-1.27),但对于报告共存疾病的 T2D 个体显著升高(HR=1.36;95%CI=1.19-1.56)。根据 T2D 持续时间进行分层表明,T2D 病史≥10 年的参与者的 CRC 特异性和全因死亡率更高。这些发现在性别和种族亚组中是一致的。与之前的报告相反,预先存在的 T2D 对 CRC 患者的疾病特异性和全因生存率没有影响。只有患有额外合并症的患者,可能还有患有长 T2D 病史的患者,与 T2D 相关的死亡率更高。