Leuthardt Eric C, Voigt Jeff, Kim Albert H, Sylvester Pete
Department of Neurosurgery, Washington University School of Medicine, St. Louis, MO, USA.
Department of Biomedical Engineering, Washington University School of Medicine, St. Louis, MO, USA.
Pharmacoecon Open. 2017 Mar;1(1):53-63. doi: 10.1007/s41669-016-0003-2.
Brain laser interstitial thermal therapy (LITT) under magnetic resonance imaging (MRI) guidance has recently gained US clinical approval for the ablation of soft, neurological tissue. LITT is a minimally invasive alternative to craniotomy.
While safety and efficacy are the focus of most current LITT studies, it is unclear how acute care costs (inpatient care ± aftercare) of LITT compare to craniotomy in an academic medical center. Therefore, the purpose of this analysis is to examine these costs of using brain LITT under MRI guidance compared to craniotomy in complex anatomies.
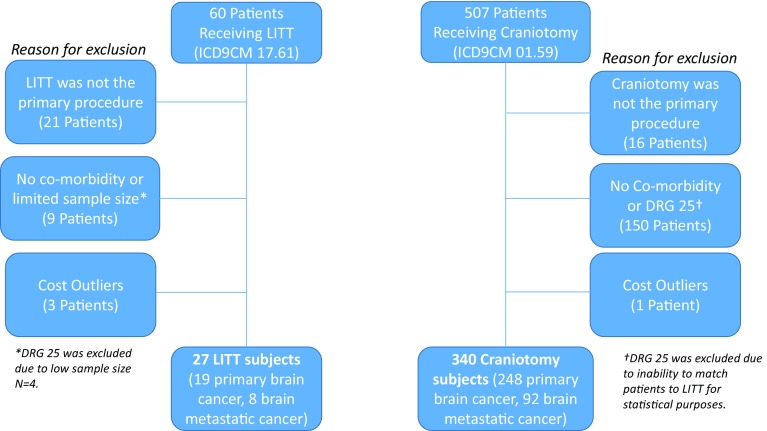
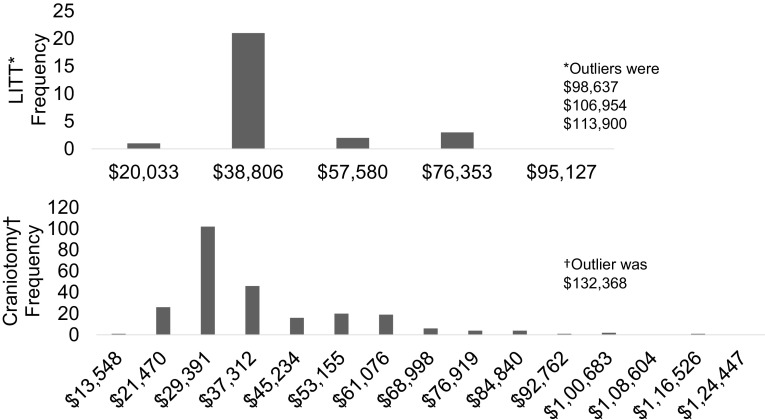
Consecutive patients treated at a single US center from 1 January 2010 to 21 October 2014 were retrospectively evaluated. Patients were included if they had a primary procedure for LITT or craniotomy (International Classification of Diseases, 9th revision, Clinical Modification [ICD-9-CM] procedure code 17.61 or ICD-9-CM procedure code 01.59, respectively) and were subgrouped according to their diagnosis of primary brain or metastatic brain cancer (ICD-9-CM 191.0-191.9 or ICD-9-CM 198.3, respectively). Patients were excluded if they had co-morbid conditions such as brain edema (ICD-9-CM 348.5). Patients were matched (LITT vs. craniotomy) based on diagnosis. Appropriate statistical analyses were undertaken to examine the year 2015 costs for care in all settings (acute hospital and post-hospital care, i.e., skilled nursing facility, rehabilitation, and home care) were examined.
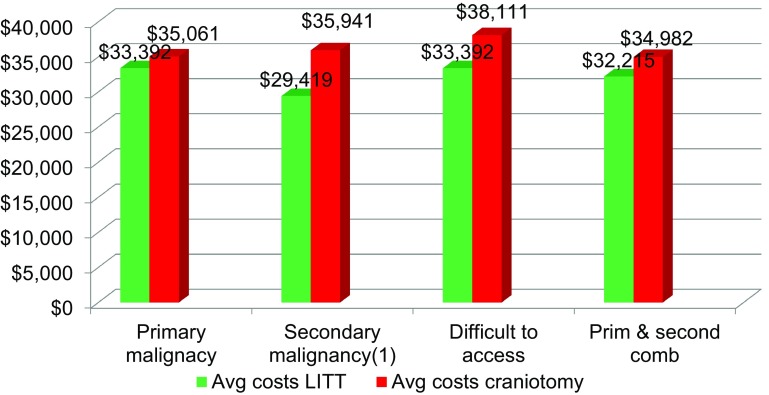
In patients treated for a primary brain cancer, there was no statistical difference in the acute and post-care costs of LITT and craniotomy (inverse variance, mean difference [MD], random effects model): MD = -US$1669; 95% confidence interval (CI) -$8192 to $4854; P = 0.62. When examining difficult to access primary malignancies, no difference was found: MD = -US$4719; 95% CI -$12,183 to $2745; P = 0.22. In metastatic brain cancer, LITT was found to be significantly less costly than craniotomy: MD = -US$6522; 95% CI -$11,911 to -$1133; P = 0.02.
In patients with metastatic brain cancer, LITT is less costly than craniotomy. Patients receiving LITT had a significantly shorter length of hospital stay, were significantly older, and were more likely to be discharged home. The use of LITT may be a reasonable option in bundled episodes of care for brain cancer and may fit into the Bundled Payment for Care Improvement (BPCI) program being evaluated by Medicare and providers.
磁共振成像(MRI)引导下的脑部激光间质热疗(LITT)最近已获得美国临床批准,用于消融软性神经组织。LITT是开颅手术的一种微创替代方法。
虽然安全性和有效性是当前大多数LITT研究的重点,但尚不清楚在学术医疗中心,LITT的急性护理成本(住院护理±术后护理)与开颅手术相比如何。因此,本分析的目的是研究在复杂解剖结构中,与开颅手术相比,MRI引导下脑部LITT的这些成本。
对2010年1月1日至2014年10月21日在美国单一中心接受治疗的连续患者进行回顾性评估。如果患者接受了LITT或开颅手术的主要手术(分别为国际疾病分类第9版临床修订本[ICD-9-CM]手术代码17.61或ICD-9-CM手术代码01.59),并根据其原发性脑癌或转移性脑癌的诊断(分别为ICD-9-CM 191.0-191.9或ICD-9-CM 198.3)进行亚组划分,则纳入研究。如果患者有脑水肿等合并症(ICD-9-CM 348.5),则排除在外。根据诊断对患者进行匹配(LITT与开颅手术)。进行了适当的统计分析,以检查2015年所有环境(急性医院和出院后护理,即熟练护理设施、康复和家庭护理)的护理成本。
在接受原发性脑癌治疗的患者中,LITT和开颅手术的急性和术后护理成本无统计学差异(逆方差,平均差异[MD],随机效应模型):MD = -1669美元;95%置信区间(CI)-8192美元至4854美元;P = 0.62。在检查难以触及的原发性恶性肿瘤时,未发现差异:MD = -4719美元;95%CI -12183美元至2745美元;P = 0.22。在转移性脑癌中,发现LITT的成本明显低于开颅手术:MD = -6522美元;95%CI -11911美元至-1133美元;P = 0.02。
在转移性脑癌患者中,LITT的成本低于开颅手术。接受LITT治疗的患者住院时间明显缩短,年龄明显较大,并更有可能出院回家。在脑癌综合护理中,使用LITT可能是一个合理的选择,并且可能符合医疗保险和提供者正在评估的改善护理综合支付(BPCI)计划。