Sullivan Rebecca, McGirr Rebecca, Hu Shirley, Tan Alice, Wu Derek, Charron Carlie, Lalonde Tyler, Arany Edith, Chakrabarti Subrata, Luyt Leonard, Dhanvantari Savita
Imaging Research, Lawson Health Research Institute, London, Ontario N6A 4V2, Canada.
Department of Pathology and Laboratory Medicine, Western University, London, Ontario N6A 4V2, Canada.
J Endocr Soc. 2017 Dec 28;2(2):178-189. doi: 10.1210/js.2017-00433. eCollection 2018 Feb 1.
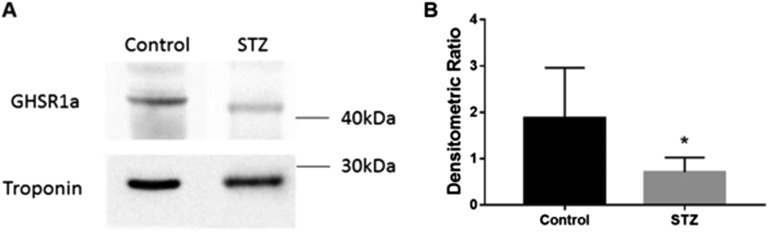
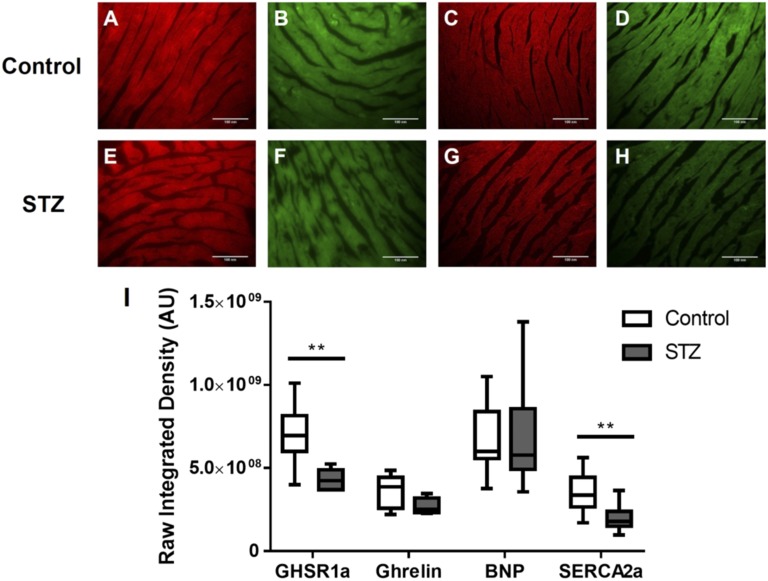
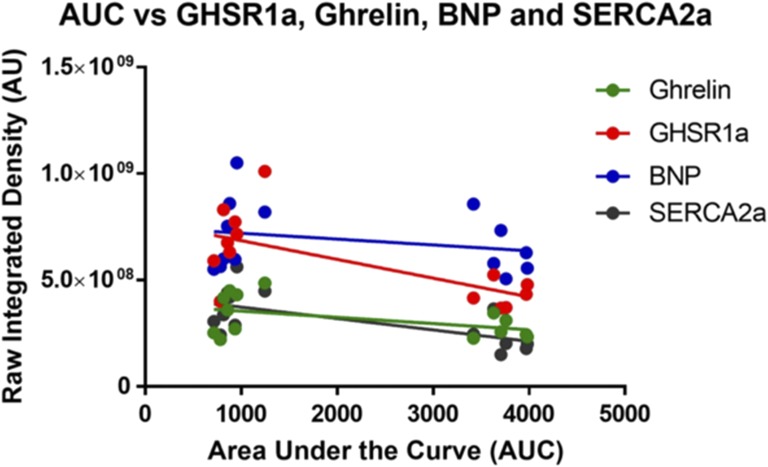
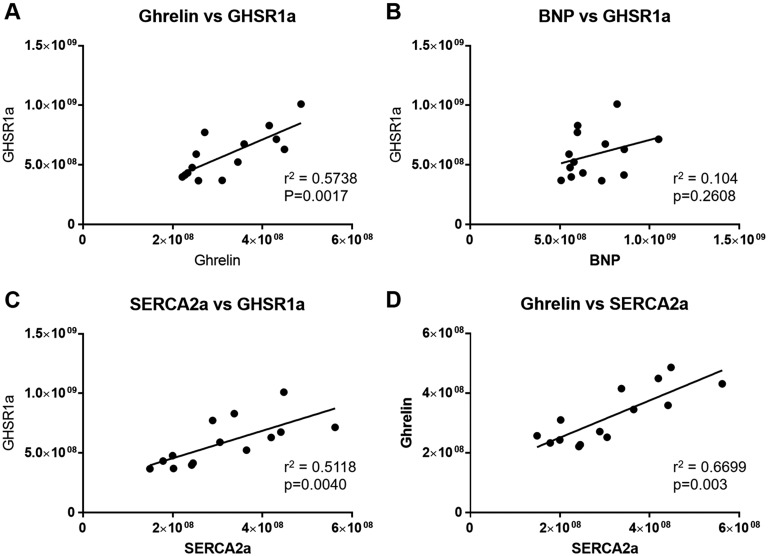
Ghrelin and its receptor, the growth hormone secretagogue receptor 1a (GHSR1a), are present in cardiac tissue. Activation of GHSR1a by ghrelin promotes cardiomyocyte contractility and survival, and changes in myocardial GHSR1a and circulating ghrelin track with end-stage heart failure, leading to the hypothesis that GHSR1a is a biomarker for heart failure. We hypothesized that GHSR1a could also be a biomarker for diabetic cardiomyopathy (DCM). We used two models of streptozotocin (STZ)-induced DCM: group 1, adult mice treated with 35 mg/kg STZ for 3 days; and group 2, neonatal mice treated with 70 mg/kg STZ at days 2 and 5 after birth. In group 1, mild fasting hyperglycemia (11 mM) was first detected 8 weeks after the last injection, and in group 2, severe fasting hyperglycemia (20 mM) was first detected 1 to 3 weeks after the last injection. In group 1, left ventricular function was slightly impaired as measured by echocardiography, and Western blot analysis showed a significant decrease in myocardial GHSR1a. In group 2, GHSR1a levels were also decreased as assessed by Cy5-ghrelin(1-19) fluorescence microscopy, and there was a significant negative correlation between GHSR1a levels and glucose tolerance. There were significant positive correlations between GHSR1a and ghrelin and between GHSR1a and sarcoplasmic reticulum Ca-ATPase 2a (SERCA2a), a marker for contractility, but not between GHSR1a and B-type natriuretic peptide, a marker for heart failure. We conclude that the subclinical stage of DCM is accompanied by alterations in the myocardial ghrelin-GHSR1a system, suggesting the possibility of a biomarker for DCM.
胃饥饿素及其受体——生长激素促分泌素受体1a(GHSR1a)存在于心脏组织中。胃饥饿素激活GHSR1a可促进心肌细胞收缩力和存活,且心肌GHSR1a和循环胃饥饿素的变化与终末期心力衰竭相关,从而产生了GHSR1a是心力衰竭生物标志物的假说。我们推测GHSR1a也可能是糖尿病性心肌病(DCM)的生物标志物。我们使用了两种链脲佐菌素(STZ)诱导的DCM模型:第1组,成年小鼠接受35 mg/kg STZ治疗3天;第2组,新生小鼠在出生后第2天和第5天接受70 mg/kg STZ治疗。在第1组中,末次注射后8周首次检测到轻度空腹高血糖(11 mM),在第2组中,末次注射后1至3周首次检测到重度空腹高血糖(20 mM)。在第1组中,通过超声心动图测量发现左心室功能略有受损,蛋白质印迹分析显示心肌GHSR1a显著降低。在第2组中,通过Cy5-胃饥饿素(1-19)荧光显微镜评估发现GHSR1a水平也降低,且GHSR1a水平与葡萄糖耐量之间存在显著负相关。GHSR1a与胃饥饿素之间以及GHSR1a与收缩力标志物肌浆网Ca-ATP酶2a(SERCA2a)之间存在显著正相关,但GHSR1a与心力衰竭标志物B型利钠肽之间无显著正相关。我们得出结论,DCM的亚临床阶段伴有心肌胃饥饿素-GHSR1a系统的改变,提示其有可能作为DCM的生物标志物。