Schmidt Christian, Öner Alper, Mann Miriam, Krockenberger Katja, Abbondanzieri Melanie, Brandewiede Bernard, Brüge Armin, Hostenkamp Gisela, Kaiser Axel, Neumeyer Henriette, Ziegler Andreas
Universitätsmedizin Rostock, Ernst-Heydemann-Str. 8, 18057, Rostock, Germany.
Abteilung Kardiologie, Universitätsmedizin Rostock, Ernst-Heydemann-Str. 8, 18057, Rostock, Germany.
Trials. 2018 Feb 20;19(1):120. doi: 10.1186/s13063-018-2502-1.
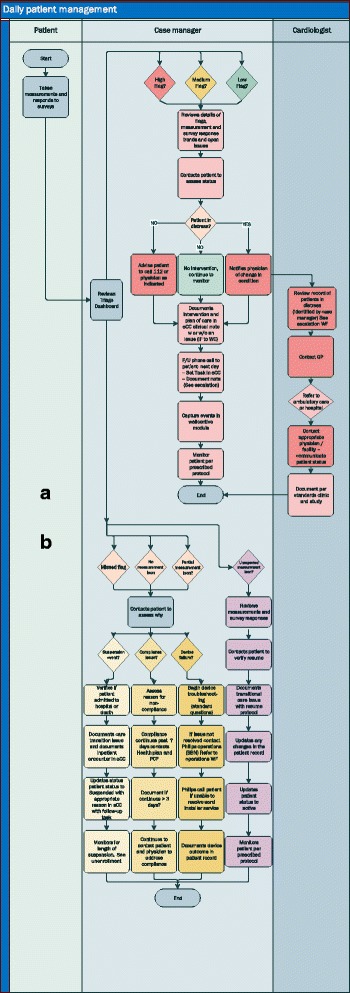
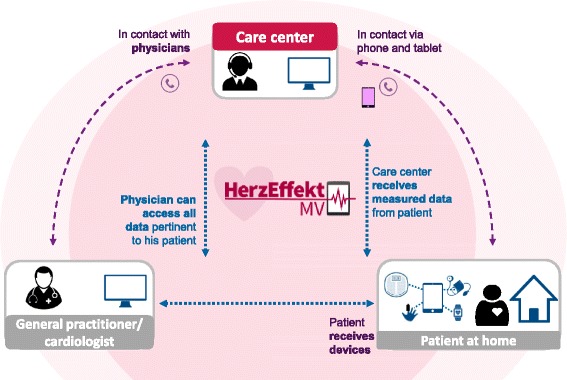
Cardiovascular diseases are the major cause of death globally and represent a major economic burden on health care systems. Positive effects of disease management programs have been shown for patients with heart failure (HF). Remote monitoring and telemonitoring with active intervention are beneficial in atrial fibrillation (AF) and therapy-resistant hypertension (TRH), respectively. For these patients, we have developed a novel integrated care concept (NICC) which combines telemedicine with intensive support by a care center, including a call center, an integrated care network including inpatient and outpatient care providers and guideline therapy for patients.
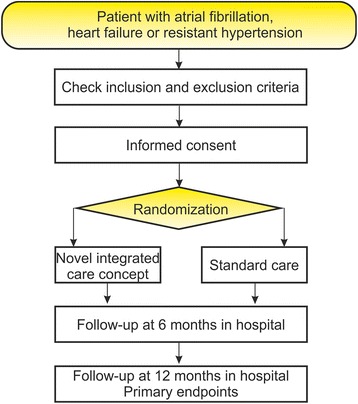
The aim of the study is to demonstrate the superiority of NICC over guideline therapy alone. The trial is designed as open-label, bi-center, parallel-group design with two groups and a blinded observer. Patients will be included if they are either inpatients or if they are referred to the outpatient clinic of the hospitals by their treating physician. Randomization will be done individually with stratification by cardiovascular disease (AF, HF, TRH), center and admission type. Primary endpoints are based on the 1-year observation period after randomization. The first primary endpoint is the composite endpoint consisting of mortality, stroke and myocardial infarction. The number of hospitalizations form the second primary endpoint. The third primary endpoint is identical to the first primary endpoint plus cardiac decompensation. Adjustments for multiple testing are done using a fall-back strategy. Secondary endpoints include patient adherence, health care costs, quality of life, and safety. A sample size of 2930 gives 80% power at the two-sided 2.5% test level for the first primary endpoint. The power for the second primary endpoint is 99.8% at this sample size, and it is 80% with 1086 patients.
This study will inform care providers whether quality of care can be improved by an integrated care concept providing telemedicine through a round-the-clock call center approach. We expect that cost of the NICC will be lower than standard care because of reduced hospitalizations. If the study has a positive result, NICC is planned to be immediately rolled out in the federal state of Mecklenburg-West Pomerania and other federal states in Germany. The trial will also guide additional research to disentangle the effects of this complex intervention.
DRKS, ID: DRKS00013124 . Registered on 5 October 2017; ClinicalTrials.gov , ID: NCT03317951. Registered on 17 October 2017.
心血管疾病是全球主要的死亡原因,也是医疗保健系统的主要经济负担。疾病管理项目已被证明对心力衰竭(HF)患者有积极作用。远程监测和带有主动干预的远程监控分别对心房颤动(AF)和难治性高血压(TRH)有益。对于这些患者,我们开发了一种新型综合护理概念(NICC),它将远程医疗与护理中心的强化支持相结合,护理中心包括一个呼叫中心、一个包括住院和门诊护理提供者的综合护理网络以及针对患者的指南治疗。
本研究的目的是证明NICC优于单纯的指南治疗。该试验设计为开放标签、双中心、平行组设计,分为两组并有一名盲法观察者。如果患者是住院患者或由其主治医生转诊至医院门诊,则将被纳入研究。随机分组将根据心血管疾病(AF、HF、TRH)、中心和入院类型进行分层,单独进行。主要终点基于随机分组后的1年观察期。第一个主要终点是由死亡率、中风和心肌梗死组成的复合终点。住院次数构成第二个主要终点。第三个主要终点与第一个主要终点相同,再加上心脏失代偿。使用后备策略对多重检验进行调整。次要终点包括患者依从性、医疗保健成本、生活质量和安全性。样本量为2930时,对于第一个主要终点,在双侧2.5%检验水平下功效为80%。在此样本量下,第二个主要终点的功效为99.8%,对于1086名患者,功效为80%。
本研究将告知护理提供者,通过全天候呼叫中心方式提供远程医疗的综合护理概念是否能提高护理质量。我们预计,由于住院次数减少,NICC的成本将低于标准护理。如果研究结果为阳性,计划在德国梅克伦堡-前波美拉尼亚州和其他联邦州立即推广NICC。该试验还将指导进一步的研究,以厘清这种复杂干预措施的效果。
德国临床试验注册中心,编号:DRKS00013124。于2017年10月5日注册;美国国立医学图书馆临床试验注册中心,编号:NCT03317951。于2017年10月17日注册。