Jönsson L, Stenvall A, Mattsson E, Larsson E, Sundlöv A, Ohlsson T, Hindorf C
Department of Medical Radiation Physics, Clinical Sciences, Lund University, Lund, Sweden.
Department of Hospital Physics, County Hospital Ryhov, Jönköping, Sweden.
EJNMMI Phys. 2018 Feb 20;5(1):5. doi: 10.1186/s40658-018-0204-0.
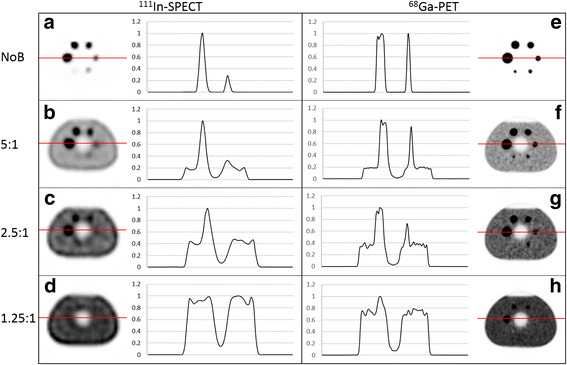
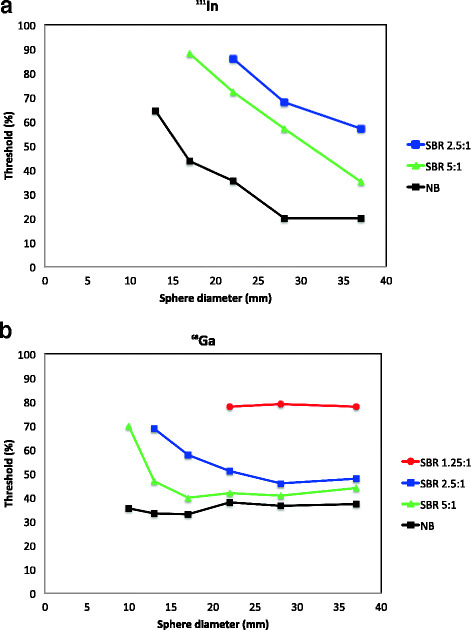
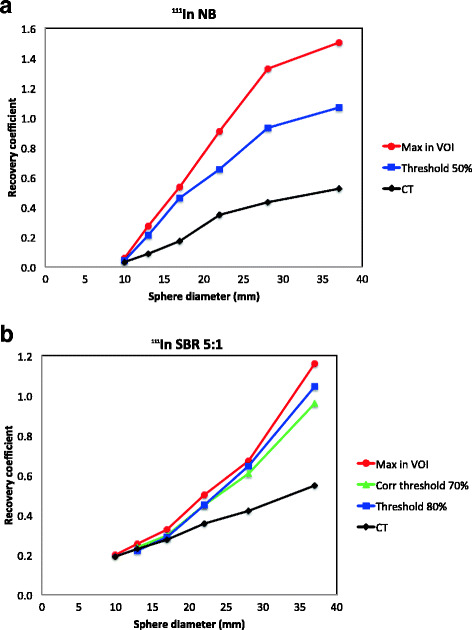
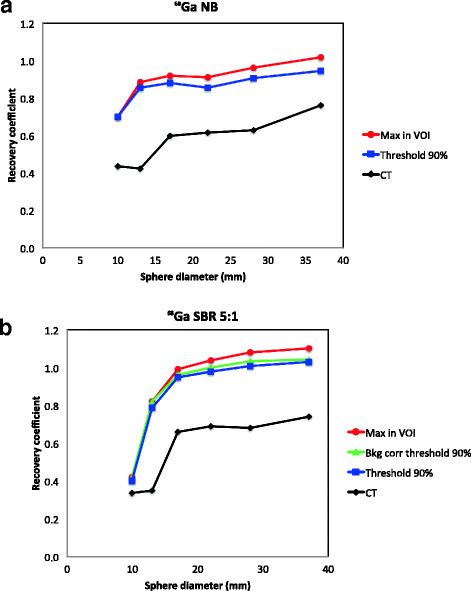
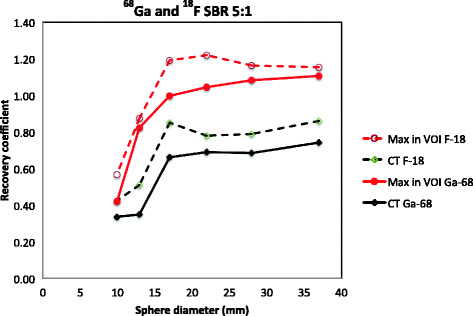
Nuclear medicine imaging of neuroendocrine tumours is performed either by SPECT/CT imaging, using In-octreotide or by PET/CT imaging using Ga-radiolabelled somatostatin analogs. These imaging techniques will give different image quality and different detection thresholds for tumours, depending on size and activity uptake. The aim was to evaluate the image quality for In-SPECT and Ga-PET imaging, i.e. the smallest volume possible to visualize for different source-to-background activity ratios. The accuracy of quantification of lesion volume and activity was also investigated to develop an objective evaluation for radionuclide therapy eligibility. The phantom study was performed using the NEMA IEC Body Phantom with six hot spheres having inner diameters of 10, 13, 17, 22, 28, and 37 mm, filled with either Ga or In with sphere-to-background ratios (SBRs) of no background activity, 5:1, 2.5:1, and 1.25:1. Activity ratios of 1.25:1 and 2.5:1 are clinically found for lesions close to the liver and spleen. Clinical acquisition and reconstruction protocols were applied. Line profiles were drawn to evaluate the smallest detectable volume within a given SBR. Recovery curves based on threshold-based VOIs, threshold-based VOIs adapted to the background and CT-based ROIs were obtained for all SBRs and sphere diameters, allowing for quantification.
The 10-mm sphere was not possible to detect in SPECT images. It was detectable in PET images for SBRs of 2.5:1 and higher. In a background corresponding to the activity uptake in the liver, spheres larger than 22-37 mm were detectable in the In-SPECT images and spheres larger than 13-22 mm were detectable in the Ga-PET images. The maximum activity concentration was accurately quantified for spheres larger than 22 mm in the PET images; however, the quantification was impaired by sphere size and background activity.
It was not possible to detect the 10-mm sphere in any of the SPECT images. In a background corresponding to the activity uptake in the liver, spheres larger than approximately 30 mm were visible in the In-SPECT images and spheres larger than approximately 17 mm were visible in the Ga-PET images. Sphere diameter and background activity strongly affect the possibility of a correct quantification.
神经内分泌肿瘤的核医学成像可通过使用铟 - 奥曲肽的SPECT/CT成像或使用镓标记的生长抑素类似物的PET/CT成像来进行。这些成像技术会因肿瘤的大小和摄取活性而产生不同的图像质量和不同的肿瘤检测阈值。目的是评估铟 - SPECT和镓 - PET成像的图像质量,即针对不同的源与背景活性比可可视化的最小体积。还研究了病变体积和活性定量的准确性,以制定放射性核素治疗适用性的客观评估。使用NEMA IEC体模进行体模研究,体模中有六个热球,内径分别为10、13、17、22、28和37毫米,填充有镓或铟,球与背景比(SBR)分别为无背景活性、5:1、2.5:1和1.25:1。临床上在靠近肝脏和脾脏的病变中发现活性比为1.25:1和2.5:1。应用了临床采集和重建方案。绘制线轮廓以评估给定SBR内的最小可检测体积。针对所有SBR和球直径,获得了基于阈值的感兴趣区(VOI)、适应背景的基于阈值的VOI以及基于CT的感兴趣区(ROI)的恢复曲线,从而实现定量。
10毫米的球在SPECT图像中无法检测到。在PET图像中,对于SBR为2.5:1及更高时可检测到。在与肝脏摄取活性相对应的背景中,铟 - SPECT图像中可检测到直径大于22 - 37毫米的球,镓 - PET图像中可检测到直径大于13 - 22毫米的球。PET图像中直径大于22毫米的球的最大活性浓度得到了准确量化;然而,量化受到球大小和背景活性的影响。
在任何SPECT图像中都无法检测到10毫米的球。在与肝脏摄取活性相对应的背景中,铟 - SPECT图像中可见直径大于约30毫米的球,镓 - PET图像中可见直径大于约17毫米的球。球直径和背景活性强烈影响正确定量的可能性。