Ball Graeme, Xie Feng, Tarride Jean-Eric
McMaster University Department of Health Research Methods, Evidence, and Impact, Faculty of Health Sciences, Hamilton, ON, Canada.
Program for Health Economics and Outcome Measures, St. Joseph's Healthcare, Hamilton, ON, Canada.
Pharmacoecon Open. 2018 Mar;2(1):19-29. doi: 10.1007/s41669-017-0030-7.
Ovarian cancer is a leading cause of cancer-related mortality. Although the disease is relatively rare, it carries a disproportionately large morbidity burden.
We conducted a cost-utility analysis from a Canadian public payer perspective to determine the cost effectiveness of bevacizumab, a newly available treatment option for recurrent ovarian cancer.
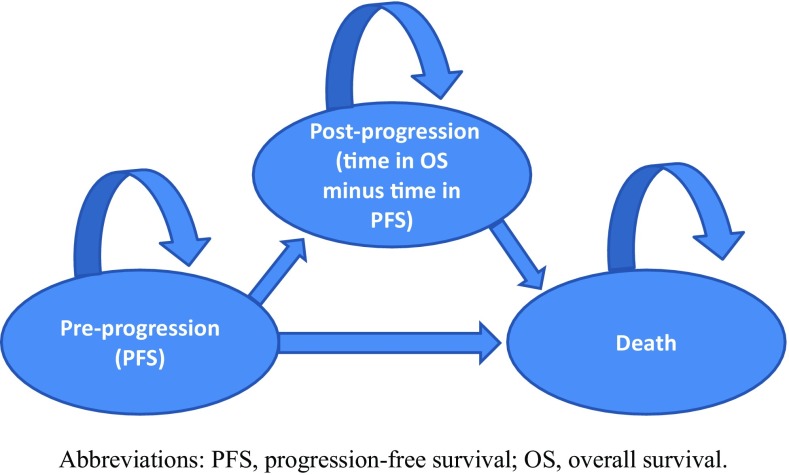
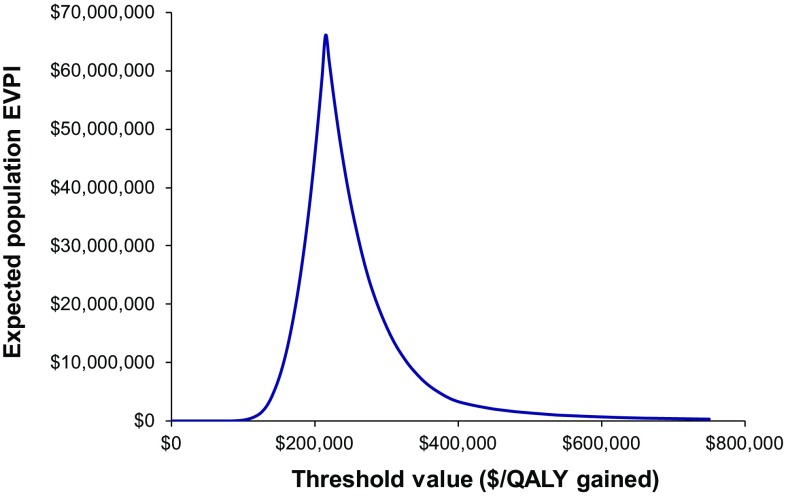
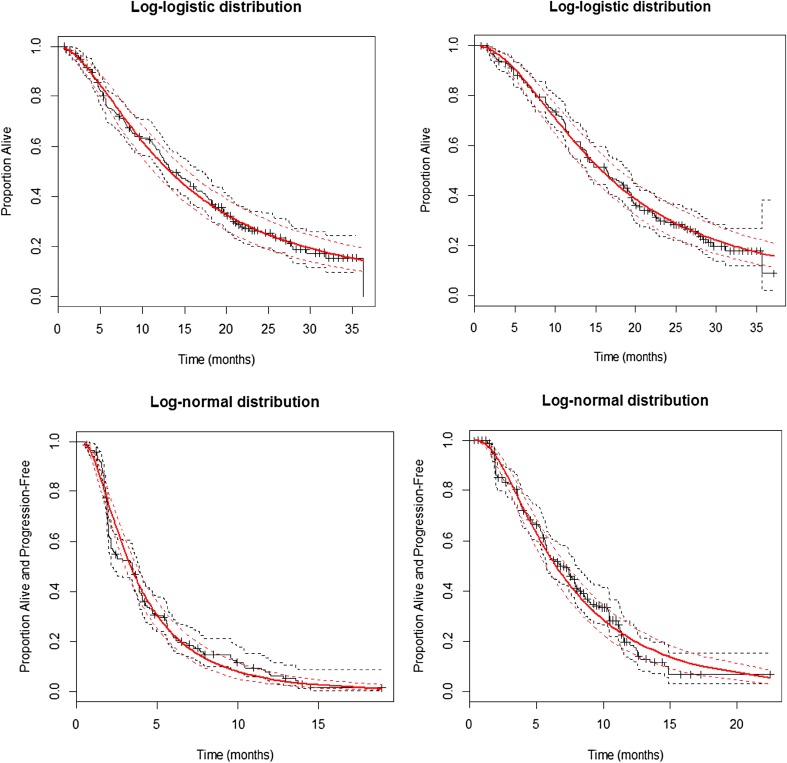
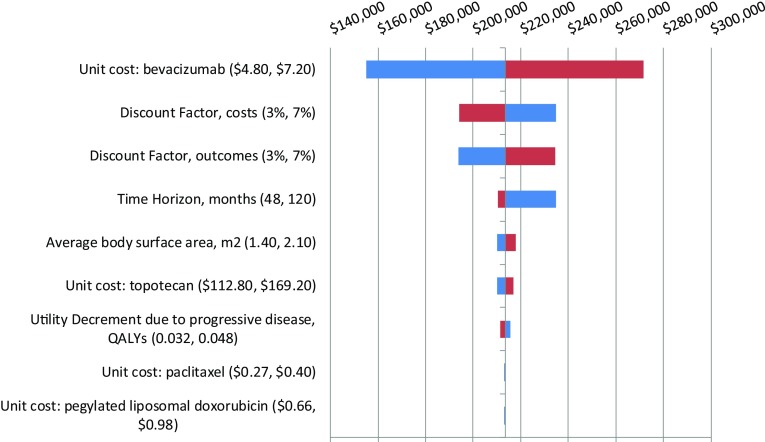
Using a 7-year time horizon, a three health-state cohort-based partitioned survival model was developed to assess the cost utility of bevacizumab plus chemotherapy (BEV) versus chemotherapy alone. We reconstructed individual patient data from published Kaplan-Meier curves. Clinical parameters, including progression-free survival and overall survival, were derived from the AURELIA phase III randomized controlled trial. Costs, resource utilization and utility values from recent Canadian sources were used to populate the model. Results were presented using incremental cost-utility ratios (ICURs). Uncertainty was examined through univariate and probabilistic sensitivity analyses.
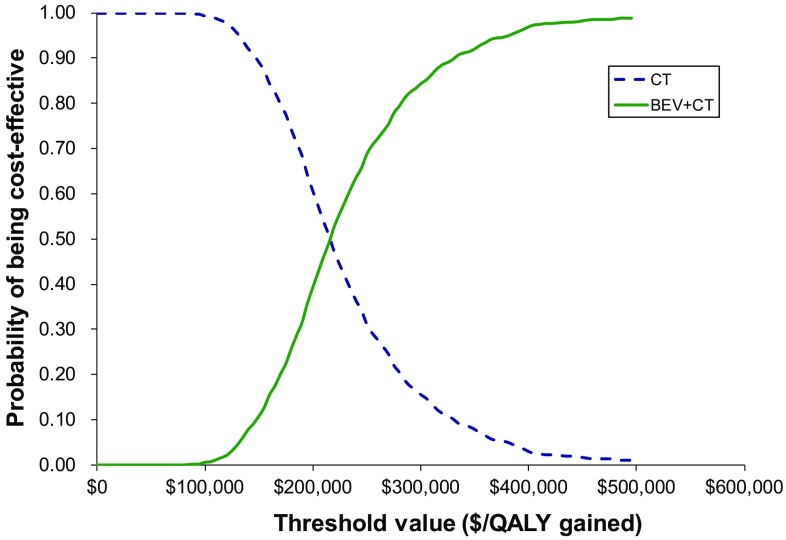
The reconstructed individual patient data matched the AURELIA trial results. Total costs for the BEV and chemotherapy treatment arms were $Can79,086 and $Can54,982, respectively. Total estimated quality-adjusted life-years (QALYs) were 1.1055 and 0.9926 for the BEV and chemotherapy arms, respectively. The ICUR was estimated to be $Can213,424 per QALY gained. At a willingness-to-pay threshold of $Can100,000 per QALY gained, the probability of BEV being cost effective was 0.
The results of our analysis suggest that the addition of bevacizumab to single-agent chemotherapy treatment, while improving patient outcomes, is unlikely to be cost effective in this Canadian patient population. The results also provide some preliminary validation for use of individual patient data-reconstruction techniques in pharmacoeconomic evaluation.
卵巢癌是癌症相关死亡的主要原因。尽管该疾病相对罕见,但它所带来的发病负担却 disproportionately 地大。
我们从加拿大公共支付者的角度进行了成本效用分析,以确定贝伐单抗(一种新的复发性卵巢癌治疗选择)的成本效益。
采用 7 年的时间范围,开发了一个基于三个健康状态队列的分区生存模型,以评估贝伐单抗联合化疗(BEV)与单纯化疗的成本效用。我们从已发表的 Kaplan-Meier 曲线中重建了个体患者数据。临床参数,包括无进展生存期和总生存期,来自 AURELIA 三期随机对照试验。使用来自加拿大近期来源的成本、资源利用和效用值来填充模型。结果以增量成本效用比(ICURs)呈现。通过单变量和概率敏感性分析来检验不确定性。
重建的个体患者数据与 AURELIA 试验结果相符。BEV 和化疗治疗组的总成本分别为 79,086 加元和 54,982 加元。BEV 和化疗组的总估计质量调整生命年(QALYs)分别为 1.1055 和 0.9926。估计的 ICUR 为每获得一个 QALY 213,424 加元。在每获得一个 QALY 支付意愿阈值为 100,000 加元时,BEV 具有成本效益的概率为 0。
我们的分析结果表明,在单药化疗治疗中添加贝伐单抗,虽然改善了患者预后,但在该加拿大患者群体中不太可能具有成本效益。这些结果也为在药物经济学评估中使用个体患者数据重建技术提供了一些初步验证。