Nafati C, Gardette M, Leone M, Reydellet L, Blasco V, Lannelongue A, Sayagh F, Wiramus S, Antonini F, Albanèse J, Zieleskiewicz L
Department of Anesthesia and Intensive Care Medicine, University Hospital of Marseille, la Timone Hospital, Marseille, France.
Service d'anesthésie et de réanimation, CHU de la Timone, 264 rue Saint Pierre, 13005, Marseille, France.
Ann Intensive Care. 2018 Feb 21;8(1):29. doi: 10.1186/s13613-018-0376-8.
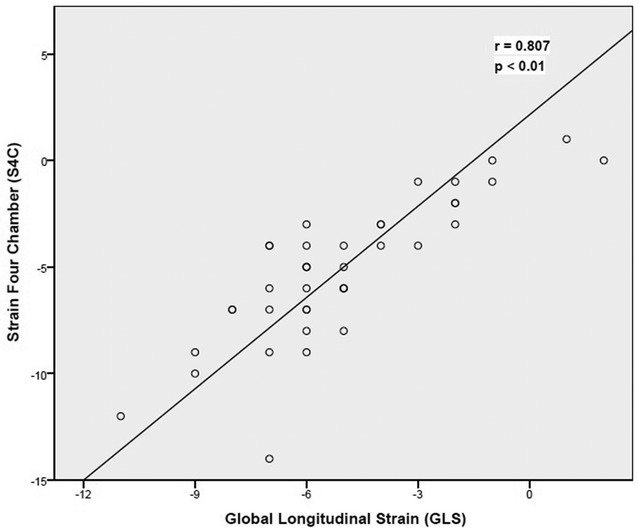
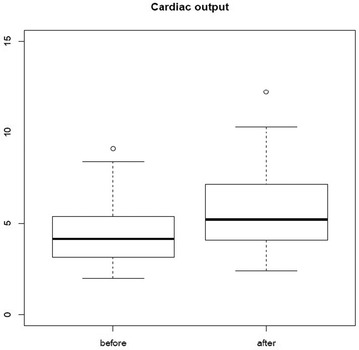
In critical patients, left ventricular ejection fraction and fractional shortening are used to reflect left ventricular systolic function. An emerging technique, two-dimensional-strain echocardiography, allows assessment of the left ventricle systolic longitudinal deformation (global longitudinal strain) and the speed at which this deformation occurs (systolic strain rate). This technique is of increasing use in critical patients in intensive care units and in the peri-operative period where preload constantly varies. Our objective, in this prospective single-center observational study, was to evaluate the effect of fluid resuscitation on two-dimensional-strain echocardiography measurements in preload-dependent critically ill patients. We included 49 patients with preload dependence attested by an increase of at least 10% in the left ventricular outflow track velocity-time integral measured by echocardiography during a passive leg raising maneuver. Echocardiography was performed before fluid resuscitation (echocardiography 1) and after preload independency achievement (echocardiography 2).
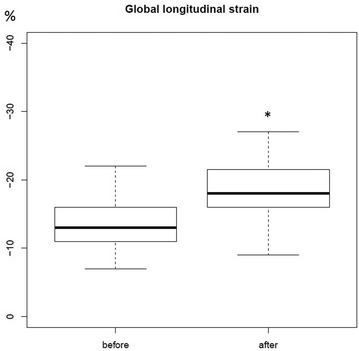
Two-dimensional-strain echocardiography was feasible in 40 (82%) among the 49 patients. With preload dependence correction, the absolute value of global longitudinal strain and systolic strain rate was significantly increased from, respectively, - 13.3 ± 3.5 to - 18.4% ± 4.5 (p < 0.01) and - 1.11 s ± 0.29 to - 1.55 s ± 0.55 (p < 0.001). The fluid resuscitation affects GLS and SSR in preload-dependent patients, with a shift, for GLS, from pathological to normal values.
In critically ill patients, the assessment of the systolic function by two-dimensional-strain echocardiography needs prior evaluation of preload dependency, in order to adequately interpret this variable. Future studies should assess the ability of global longitudinal strain to guide fluid management in the critically ill patients.
在危重症患者中,左心室射血分数和缩短分数用于反映左心室收缩功能。一种新兴技术,二维应变超声心动图,能够评估左心室收缩期纵向变形(整体纵向应变)以及这种变形发生的速度(收缩期应变率)。在重症监护病房的危重症患者以及围手术期,前负荷不断变化,这项技术的应用越来越广泛。在这项前瞻性单中心观察性研究中,我们的目的是评估液体复苏对前负荷依赖型危重症患者二维应变超声心动图测量结果的影响。我们纳入了49例在前负荷依赖方面有证据的患者,证据是在被动抬腿试验期间通过超声心动图测量左心室流出道速度时间积分至少增加10%。在液体复苏前(超声心动图1)和达到前负荷非依赖状态后(超声心动图2)进行超声心动图检查。
49例患者中有40例(82%)可行二维应变超声心动图检查。随着前负荷依赖的纠正,整体纵向应变和收缩期应变率的绝对值分别从-13.3±3.5显著增加至-18.4%±4.5(p<0.01)和-1.11 s±0.29至-1.55 s±0.55(p<0.)。液体复苏影响前负荷依赖型患者的整体纵向应变(GLS)和收缩期应变率(SSR),对于GLS而言,从病理值转变为正常范围。
在危重症患者中,通过二维应变超声心动图评估收缩功能需要事先评估前负荷依赖性,以便充分解读这一变量。未来的研究应评估整体纵向应变指导危重症患者液体管理的能力。