Wasson John H, Ho Lynn, Soloway Laura, Moore L Gordon
Centers for Health and Aging, Dartmouth Medical School, Lebanon, NH, United States of America.
North Kingstown Family Practice, North Kingstown, RI, United States of America.
PLoS One. 2018 Feb 22;13(2):e0192475. doi: 10.1371/journal.pone.0192475. eCollection 2018.
Current health care delivery relies on complex, computer-generated risk models constructed from insurance claims and medical record data. However, these models produce inaccurate predictions of risk levels for individual patients, do not explicitly guide care, and undermine health management investments in many patients at lesser risk. Therefore, this study prospectively validates a concise patient-reported risk assessment that addresses these inadequacies of computer-generated risk models.
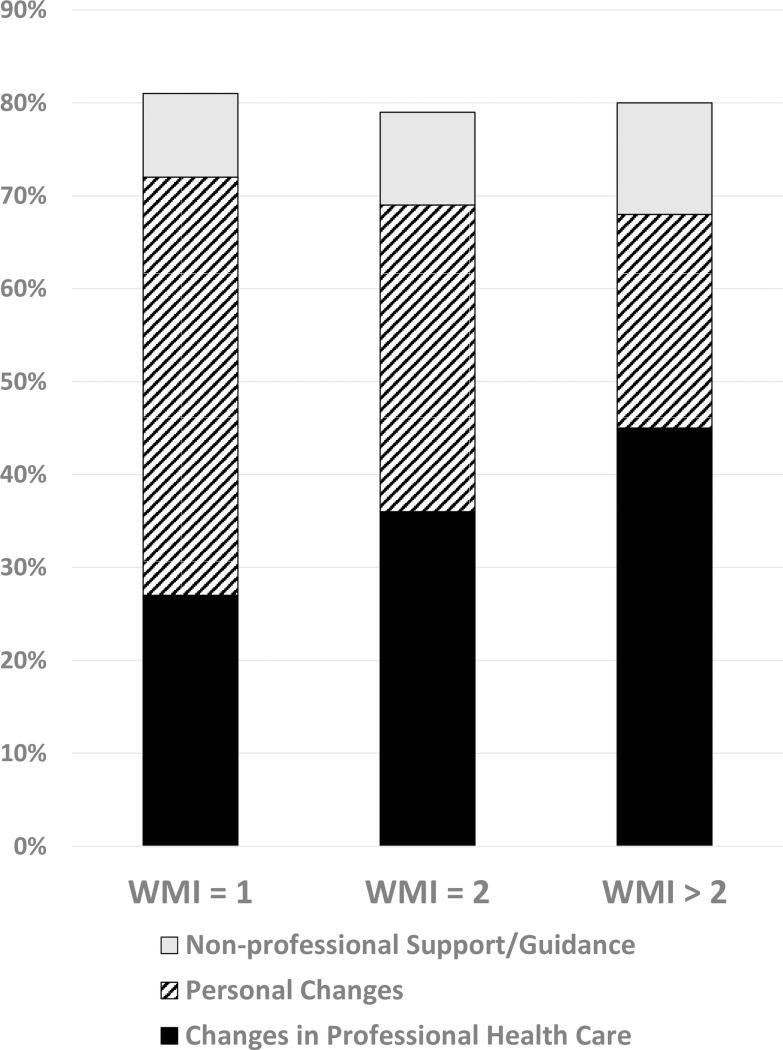
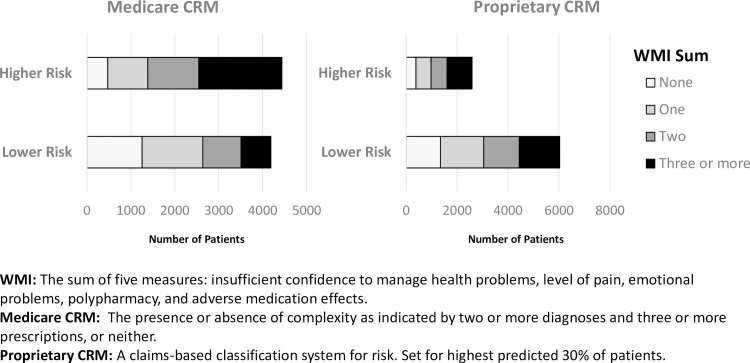
Five measures with well-documented impacts on the use of health services are summed to create a "What Matters Index." These measures are: 1) insufficient confidence to self-manage health problems, 2) pain, 3) bothersome emotions, 4) polypharmacy, and 5) adverse medication effects. We compare the sensitivity and predictive values of this index with two representative risk models in a population of 8619 Medicaid recipients.
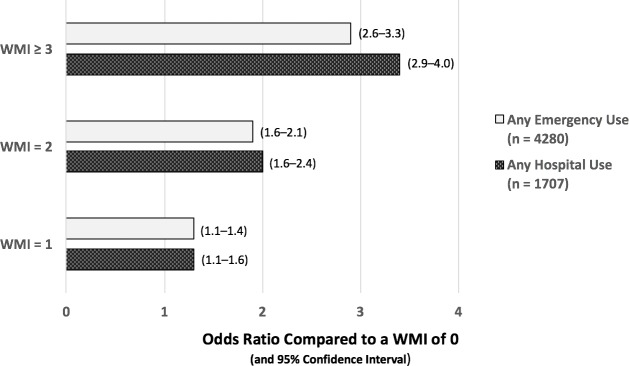
The patient-reported "What Matters Index" and the conventional risk models are found to exhibit similar sensitivities and predictive values for subsequent hospital or emergency room use. The "What Matters Index" is also reliable: akin to its performance during development, for patients with index scores of 1, 2, and ≥3, the odds ratios (with 95% confidence intervals) for subsequent hospitalization within 1 year, relative to patients with a score of 0, are 1.3 (1.1-1.6), 2.0 (1.6-2.4), and 3.4 (2.9-4.0), respectively; for emergency room use, the corresponding odds ratios are 1.3 (1.1-1.4), 1.9 (1.6-2.1), and 2.9 (2.6-3.3). Similar findings were replicated among smaller populations of 1061 mostly older patients from nine private practices and 4428 Medicaid patients without chronic conditions.
In contrast to complex computer-generated risk models, the brief patient-reported "What Matters Index" immediately and unambiguously identifies fundamental, remediable needs for each patient and more sensibly directs the delivery of services to patient categories based on their risk for subsequent costly care.
当前的医疗服务依赖于由保险理赔和病历数据构建的复杂计算机生成风险模型。然而,这些模型对个体患者的风险水平预测不准确,不能明确指导治疗,并且削弱了对许多低风险患者的健康管理投资。因此,本研究前瞻性地验证了一种简洁的患者报告风险评估方法,以解决计算机生成风险模型的这些不足。
将五项对医疗服务使用有充分记录影响的指标相加,创建一个“重要事项指数”。这些指标是:1)自我管理健康问题信心不足,2)疼痛,3)烦扰情绪,4)多重用药,5)药物不良反应。我们在8619名医疗补助接受者群体中比较该指数与两种代表性风险模型的敏感性和预测值。
发现患者报告的“重要事项指数”与传统风险模型在预测后续住院或急诊室使用方面表现出相似的敏感性和预测值。“重要事项指数”也具有可靠性:与开发期间的表现类似,对于指数得分分别为1、2和≥3的患者,相对于得分为0的患者,1年内后续住院的比值比(95%置信区间)分别为1.3(1.1 - 1.6)、2.0(1.6 - 2.4)和3.4(2.9 - 4.0);对于急诊室使用,相应的比值比分别为1.3(1.1 - 1.4)、1.9(1.6 - 2.1)和2.9(2.6 - 3.3)。在来自九个私人诊所的1061名大多为老年患者的较小群体以及4428名无慢性病的医疗补助患者中也得到了类似的结果。
与复杂的计算机生成风险模型不同,简短的患者报告“重要事项指数”能立即明确识别每个患者的基本可补救需求,并根据患者后续昂贵护理的风险更合理地指导服务提供。