Cardiology Unit "Card. G. Panico" Hospital, Tricase, Italy
Cardiology and Arrhythmology Clinic, Marche Polytechnic University University Hospital "Umberto I-Lancisi-Salesi,", Ancona, Italy.
J Am Heart Assoc. 2018 Feb 24;7(5):e008146. doi: 10.1161/JAHA.117.008146.
To determine whether daily physical activity (PA), as measured by implanted devices (through accelerometer sensor), was related to the risk of developing atrial arrhythmias during long-term follow-up in a population of heart failure (HF) patients with an implantable cardioverter defibrillator (ICD).
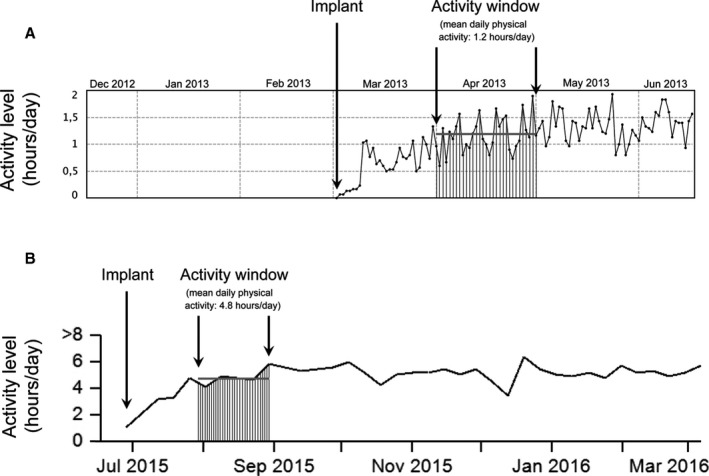
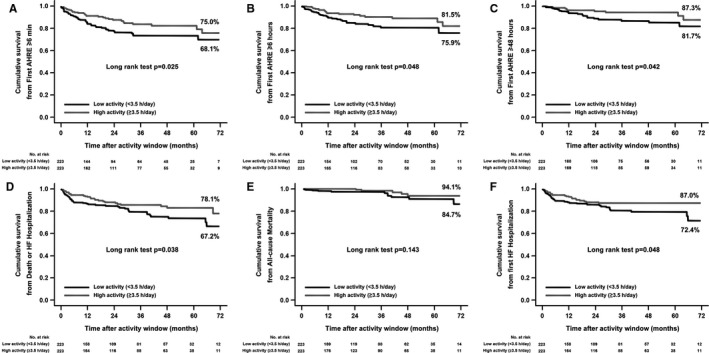
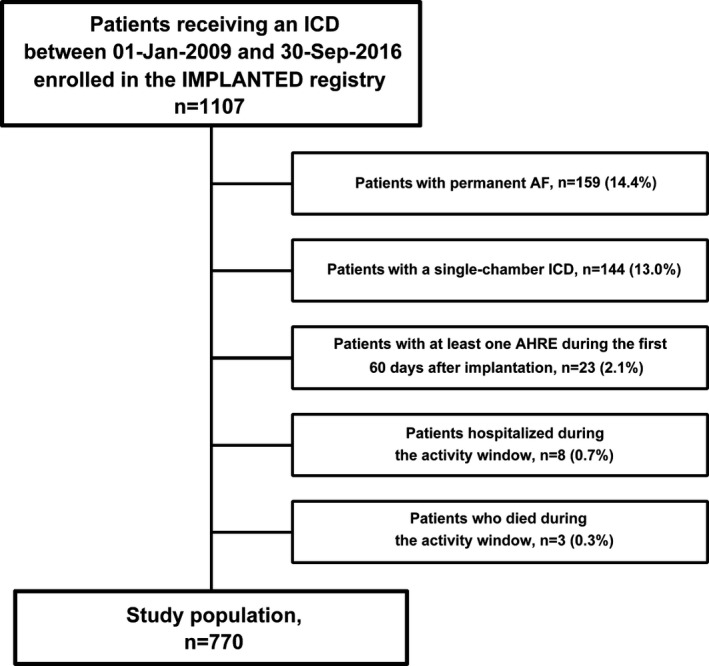
The study population was divided into 2 equally sized groups (PA cutoff point: 3.5 h/d) according to their mean daily PA recorded by the device during the 30- to 60-day period post-ICD implantation. Propensity score matching was used to compare 2 equally sized cohorts with similar characteristics between lower and higher activity patients. The primary end point was time free from the first atrial high-rate episode (AHRE) of duration ≥6 minutes. Secondary end points were: first AHRE ≥6 hours, first AHRE ≥48 hours, and a combined end point of death or HF hospitalization. Data from 770 patients (65±15 years; 66% men; left ventricular ejection fraction 35±12%) remotely monitored for a median of 25 months were analyzed. A PA ≥3.5 h/d was associated with a 38% relative reduction in the risk of AHRE ≥6 minutes (72-month cumulative survival: 75.0% versus 68.1%; log rank =0.025), and with a reduction in the risk of AHRE ≥6 hours, AHRE ≥48 hours, and the combined end point of death or HF hospitalization (all <0.05).
In HF patients with ICD, a low level of daily PA was associated with a higher risk of atrial arrhythmias, regardless of the patients' baseline characteristics. In addition, a lower daily PA predicted death or HF hospitalization.
通过植入设备(通过加速度计传感器)测量的日常体力活动(PA)是否与植入式心脏复律除颤器(ICD)植入后长期随访期间心力衰竭(HF)患者发生心房心律失常的风险相关。
根据患者植入 ICD 后 30-60 天期间设备记录的平均每日 PA,将研究人群分为两组(PA 截断点:3.5 h/d)。使用倾向评分匹配比较两组患者在低活动和高活动患者之间具有相似特征的患者。主要终点是无首次持续时间≥6 分钟的心房快速率事件(AHRE)的时间。次要终点为:首次 AHRE≥6 小时,首次 AHRE≥48 小时,以及死亡或 HF 住院的联合终点。对 770 例(65±15 岁;66%为男性;左心室射血分数 35±12%)接受中位数为 25 个月远程监测的患者数据进行了分析。PA≥3.5 h/d 与 AHRE≥6 分钟的风险降低 38%相关(72 个月累积生存率:75.0%与 68.1%;对数秩检验=0.025),并且降低了 AHRE≥6 小时,AHRE≥48 小时和死亡或 HF 住院的联合终点(均<0.05)。
在 HF 合并 ICD 的患者中,日常 PA 水平较低与心房心律失常的风险增加相关,而与患者的基线特征无关。此外,较低的日常 PA 预测死亡或 HF 住院。