Dermatology Clinic, Brussels, Belgium.
Institut de Recherche Interdisciplinaire en Biologie humaine et moléculaire (IRIBHM) & Service de Biostatistique et Informatique médicale (SBIM), Université libre de Bruxelles (ULB), Brussels, Belgium.
J Eur Acad Dermatol Venereol. 2018 Jun;32(6):1011-1016. doi: 10.1111/jdv.14885. Epub 2018 Mar 23.
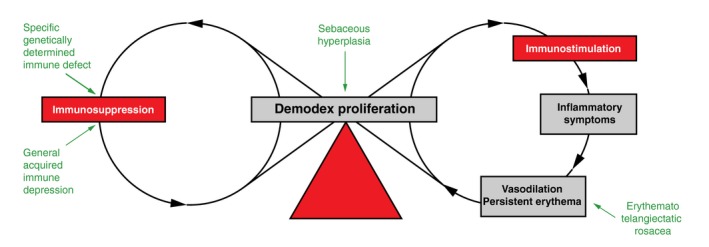
Papulopustular rosacea and rosacea-like demodicosis have numerous similarities, but they are generally considered as two distinct entities, mainly because the causal role of the Demodex mite in the development of rosacea is not yet widely accepted. Several clinical characteristics are traditionally considered to differentiate the two conditions; for example, papulopustular rosacea is typically characterized by central facial papulopustules and persistent erythema, whereas small superficial papulopustules and follicular scales rather suggest rosacea-like demodicosis. However, none of these characteristics is exclusive to either entity.
To explore differences in Demodex densities according to clinical characteristics traditionally associated with these two conditions.
Retrospective, observational, case-control study of 242 patients with central face papulopustules. Demodex densities were measured on two consecutive standardized skin surface biopsies.
In the whole cohort, Demodex densities were greater in patients with persistent erythema than in those without. In 132 patients without recent treatment or other facial dermatoses, 120 (91%) had persistent erythema, 119 (90%) small superficial papulopustules and 124 (94%) follicular scales; 116 (88%) simultaneously had clinical characteristics traditionally associated with both papulopustular rosacea and rosacea-like demodicosis. Higher Demodex densities were linked to the presence of follicular scales, but not to papulopustules size, nor to the presence/absence of persistent erythema.
Our observations highlight the difficulty differentiating between these entities and suggest that rosacea-like demodicosis and papulopustular rosacea should no longer be considered as two separate entities, but rather as two phenotypes of the same disease.
丘疹脓疱型酒渣鼻和酒渣鼻样蠕形螨病有许多相似之处,但它们通常被认为是两种不同的实体,主要是因为螨虫在酒渣鼻发展中的因果作用尚未被广泛接受。传统上有一些临床特征被认为可以区分这两种情况;例如,丘疹脓疱型酒渣鼻的典型特征是中央面部丘疹脓疱和持续性红斑,而小的浅表丘疹脓疱和滤泡鳞屑则提示酒渣鼻样蠕形螨病。然而,这些特征没有一个是这两种实体所特有的。
根据与这两种情况相关的传统临床特征,探讨螨虫密度的差异。
对 242 例中央面部丘疹脓疱患者进行回顾性、观察性、病例对照研究。在两次连续的标准化皮肤表面活检中测量螨虫密度。
在整个队列中,持续性红斑患者的螨虫密度大于无持续性红斑患者。在 132 例无近期治疗或其他面部皮肤病的患者中,120 例(91%)有持续性红斑,119 例(90%)有小的浅表丘疹脓疱,124 例(94%)有滤泡鳞屑;116 例(88%)同时具有与丘疹脓疱型酒渣鼻和酒渣鼻样蠕形螨病相关的临床特征。较高的螨虫密度与滤泡鳞屑的存在有关,但与丘疹脓疱的大小无关,也与持续性红斑的存在/不存在无关。
我们的观察结果强调了区分这两种实体的困难,并表明酒渣鼻样蠕形螨病和丘疹脓疱型酒渣鼻不应再被视为两种不同的实体,而应被视为同一种疾病的两种表型。