Department of Radiation Oncology, University Hospital, LMU Munich, Marchioninistr. 15, 81377, Munich, Germany.
Department of Nuclear Medicine, University Hospital, LMU Munich, Munich, Germany.
Radiat Oncol. 2018 Mar 2;13(1):37. doi: 10.1186/s13014-018-0983-4.
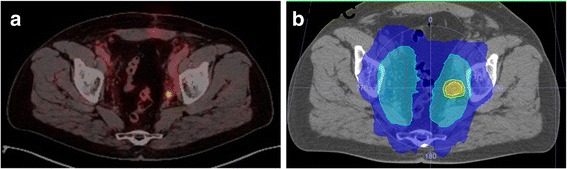
PSMA PET/CT visualises prostate cancer residual disease or recurrence at lower PSA levels compared to conventional imaging and results in a change of treatment in a remarkable high number of patients. Radiotherapy with dose escalation to the former prostate bed has been associated with improved biochemical recurrence-free survival. Thus, it can be hypothesised that PSMA PET/CT-based radiotherapy might improve the prognosis of these patients.
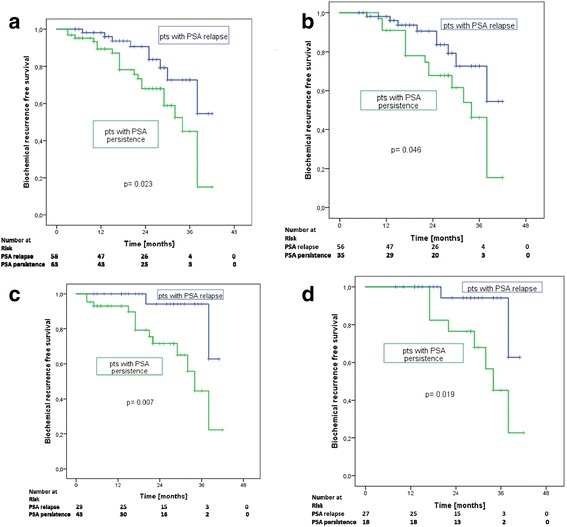
One hundred twenty-nine patients underwent PSMA PET/CT due to biochemical persistence (52%) or recurrence (48%) after radical prostatectomy without evidence of distant metastases (February 2014-May 2017) and received PSMA PET/CT-based radiotherapy. Biochemical recurrence free survival (PSA ≤ 0.2 ng/ml) was defined as the study endpoint.
Patients with biochemical persistence were significantly more often high-risk patients with significantly shorter time interval before PSMA PET/CT than patients with biochemical recurrence. Patients with biochemical recurrence had significantly more often no evidence of disease or local recurrence only in PSMA PET/CT, whereas patients with biochemical persistence had significantly more often lymph node involvement. Seventy-three patients were started on antiandrogen therapy prior to radiotherapy due to macroscopic disease in PSMA PET/CT. Cumulatively, 70 (66-70.6) Gy was delivered to local macroscopic tumor, 66 (63-66) Gy to the prostate fossa, 61.6 (53.2-66) Gy to PET-positive lymph nodes and 50.4 (45-52.3) Gy to lymphatic pathways. Median PSA after radiotherapy was 0.07 ng/ml with 74% of patients having a PSA ≤ 0.1 ng/ml. After a median follow-up of 20 months, median PSA was 0.07 ng/ml with ongoing antiandrogen therapy in 30 patients. PET-positive patients without antiandrogen therapy at last follow-up (45 patients) had a median PSA of 0.05 ng/ml with 89% of all patients, 94% of patients with biochemical recurrence and 82% of patients with biochemical persistence having a PSA ≤ 0.2 ng/ml. Post-radiotherapy PSA ≤ 0.1 ng/ml and biochemical recurrence vs. persistence were significantly associated with a PSA ≤ 0.2 ng/ml at last follow-up.
PSMA PET/CT-based radiotherapy is an effective local salvage treatment option with significant PSA response in patients with biochemical recurrence or persistence after radical prostatectomy leading to deferral of long-term ADT or systemic therapy.
与传统影像学相比,PSMA PET/CT 可在 PSA 水平较低时检测前列腺癌残留疾病或复发,导致相当数量的患者改变治疗方案。对原前列腺床进行剂量升级的放疗与生化无复发生存率的改善相关。因此,可以假设 PSMA PET/CT 引导的放疗可能改善这些患者的预后。
129 例患者因根治性前列腺切除术后生化持续存在(52%)或复发(48%)且无远处转移证据(2014 年 2 月至 2017 年 5 月)而行 PSMA PET/CT 检查,并接受 PSMA PET/CT 引导的放疗。生化无复发生存(PSA≤0.2ng/ml)被定义为研究终点。
生化持续存在的患者明显更多地为高危患者,且在进行 PSMA PET/CT 检查前的时间间隔明显短于生化复发的患者。生化复发的患者在 PSMA PET/CT 中明显更多地没有疾病或仅局部复发的证据,而生化持续存在的患者明显更多地有淋巴结受累。由于 PSMA PET/CT 中存在宏观疾病,73 例患者在放疗前开始接受抗雄激素治疗。累计向局部宏观肿瘤、前列腺窝、PSMA 阳性淋巴结和淋巴途径分别给予 70(66-70.6)Gy、66(63-66)Gy、61.6(53.2-66)Gy 和 50.4(45-52.3)Gy。放疗后中位 PSA 为 0.07ng/ml,74%的患者 PSA≤0.1ng/ml。中位随访 20 个月后,中位 PSA 为 0.07ng/ml,30 例患者持续接受抗雄激素治疗。最后一次随访时未接受抗雄激素治疗的 PET 阳性患者(45 例)PSA 中位数为 0.05ng/ml,所有患者、生化复发患者和生化持续存在患者的 94%、82%PSA≤0.2ng/ml。放疗后 PSA≤0.1ng/ml 和生化复发与持续存在与最后随访时 PSA≤0.2ng/ml 显著相关。
PSMA PET/CT 引导的放疗是一种有效的局部挽救治疗方法,在根治性前列腺切除术后生化复发或持续存在的患者中具有显著的 PSA 反应,可延迟长期 ADT 或全身治疗。