Section of Cardiac Electrophysiology, University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania; Department of Cardiology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, China.
Section of Cardiac Electrophysiology, University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania; Department of Radiology, Hospital of the University of Pennsylvania, University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania.
Heart Rhythm. 2018 Jul;15(7):987-993. doi: 10.1016/j.hrthm.2018.02.030. Epub 2018 Mar 2.
Criteria for identification of anatomic ventricular tachycardia substrates in arrhythmogenic right ventricular cardiomyopathy (ARVC) on late gadolinium enhancement (LGE) cardiac magnetic resonance (CMR) are unclear.
The purpose of this study was to define (1) the association of regional right ventricular (RV) epicardial voltage amplitude with the distribution of LGE; and (2) appropriate image signal intensity (SI) thresholds for ventricular tachycardia substrate identification in ARVC.
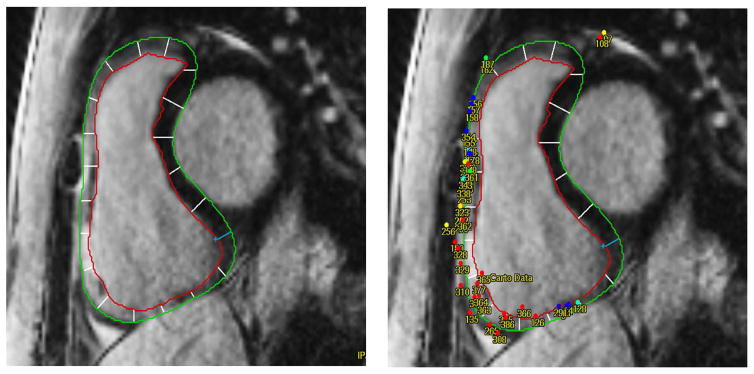
Preprocedural LGE-CMR and epicardial electrogram mapping were performed in 10 ARVC patients. The locations of epicardial electrogram map points, obtained during sinus rhythm with intrinsic conduction or RV pacing, were retrospectively registered to the corresponding LGE image regions. Standardized SI z-scores (standard deviation distance from the mean) were calculated for each 10-mm region surrounding map points.
In patient-clustered, generalized estimating equations models that included 3205 epicardial electroanatomic points and corresponding SI measures, bipolar (-1.43 mV/z-score; P <.001) and unipolar voltage amplitude (-1.22 mV/z-score; P <.001) were associated with regional SI z-scores. In contrast to the QRS-late potential (LP) interval (P = .362), the LP activation index, defined as electrogram duration divided by QRS-LP, was associated with regional SI z-scores (P <.001). SI z-score thresholds >0.05 (95% confidence interval -0.05 to 0.15) and <-0.16 (95% confidence interval -0.26 to 0.06) corresponded to bipolar voltage measures <0.5 and >1.0 mV, respectively.
Increased RV gadolinium uptake is associated with lower epicardial bipolar and unipolar electrogram voltage amplitude. Standardized LGE-CMR SI z-scores may augment preprocedural planning for identification of low-voltage zones and abnormal myocardium in ARVC.
在心律失常性右心室心肌病(ARVC)的晚期钆增强(LGE)心脏磁共振(CMR)中,识别解剖性室性心动过速基质的标准尚不清楚。
本研究的目的是定义:(1)右心室(RV)心外膜电压幅度与 LGE 分布的相关性;(2)在 ARVC 中确定室性心动过速基质的合适图像信号强度(SI)阈值。
对 10 例 ARVC 患者进行术前 LGE-CMR 和心外膜电图标测。在窦性心律下,通过固有传导或 RV 起搏获得心外膜电图标测点的位置,然后将其回顾性地注册到相应的 LGE 图像区域。为每个围绕标测点的 10mm 区域计算 SI 的标准化 Z 分数(平均值的标准偏差距离)。
在包含 3205 个心外膜电生理点和相应 SI 测量值的患者聚类广义估计方程模型中,双极(-1.43mV/Z 分数;P<0.001)和单极电压幅度(-1.22mV/Z 分数;P<0.001)与局部 SI Z 分数相关。与 QRS 晚期电位(LP)间期(P=0.362)不同,定义为电图持续时间除以 QRS-LP 的 LP 激活指数与局部 SI Z 分数相关(P<0.001)。SI Z 分数阈值>0.05(95%置信区间 -0.05 至 0.15)和<-0.16(95%置信区间 -0.26 至 0.06)分别对应于双极电压测量值<0.5 和>1.0mV。
RV 钆摄取增加与心外膜双极和单极电图电压幅度降低有关。标准化 LGE-CMR SI Z 分数可能会增强 ARVC 中识别低电压区和异常心肌的术前规划。