Zhou Bo, Zhan Canyang, Ding Yuan, Yan Sheng, Zheng Shusen
Division of Hepatobiliary and Pancreatic Surgery, Department of Surgery, First Affiliated Hospital.
Department of Neonatology, Children's Hospital, School of Medicine, Zhejiang University, Hangzhou, People's Republic of China.
Onco Targets Ther. 2018 Feb 23;11:975-982. doi: 10.2147/OTT.S158171. eCollection 2018.
Treatment for pancreatic neuroendocrine tumors (PNETs) in patients with unresectable metastatic liver disease has long been a controversial issue. This systematic review aims to summarize the existing evidence concerning the value of primary tumor resection in this group of patients.
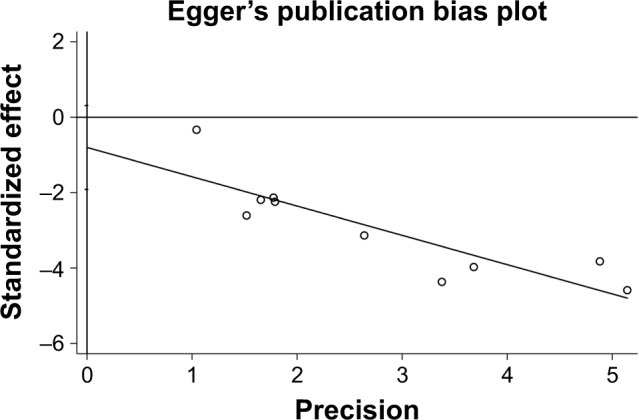
A systematic review of the literature and a meta-analysis were performed. The PubMed and Cochrane databases were searched to identify articles that compared palliative primary tumor resection and nonsurgical regimens in patients with PNETs and unresectable liver metastases. Relevant articles were identified in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The primary outcome was overall survival. The included studies were evaluated for heterogeneity and publication bias.
Overall, 10 studies were included in the analysis. No randomized controlled trials (RCTs) were identified. These studies included 1,226 patients who underwent a resection of the primary tumor and 1,623 patients who did not undergo surgery. The median overall survival was 36-137 and 13.2-65 months in the surgical and nonsurgical groups, respectively, and the 5-year overall survival rate was 35.7-83 and 5.4%-50%, respectively, in these two groups. The meta-analysis demonstrated that there was no significant difference in liver tumor burden (odds ratio [OR] =1.51, 95% CI: 0.59-3.89, =0.39) or tumor grade (OR =2.88, 95% CI: 0.92-9.04, =0.07) among patients who underwent surgery and nonsurgical therapy. Furthermore, patients who underwent an aggressive surgical approach appeared to have a higher tumor grade. However, the meta-analysis demonstrated that patients who underwent primary tumor resection had better overall survival (<0.001), with a pooled hazard ratio of 0.36 (95% CI: 0.30-0.45). No publication bias was detected.
This meta-analysis demonstrates that the palliative resection of the primary tumor in patients with PNETs and unresectable liver metastases can increase survival, although a bias toward a more aggressive surgical approach in patients with better performance status, less advanced disease, or a tumor located in the body or tail of the pancreas appears likely. RCTs with longer follow-up periods are required to confirm the advantages of palliative primary tumor resection for PNETs.
对于患有无法切除的转移性肝病的胰腺神经内分泌肿瘤(PNETs)患者的治疗,长期以来一直是一个有争议的问题。本系统评价旨在总结有关该组患者原发性肿瘤切除价值的现有证据。
进行了文献系统评价和荟萃分析。检索了PubMed和Cochrane数据库,以识别比较PNETs合并无法切除肝转移患者的姑息性原发性肿瘤切除与非手术治疗方案的文章。根据系统评价和荟萃分析的首选报告项目(PRISMA)指南识别相关文章。主要结局为总生存期。对纳入研究进行异质性和发表偏倚评估。
总体而言,10项研究纳入分析。未识别到随机对照试验(RCT)。这些研究包括1226例行原发性肿瘤切除的患者和1623例未接受手术的患者。手术组和非手术组的中位总生存期分别为36 - 137个月和13.2 - 65个月,两组的5年总生存率分别为35.7% - 83%和5.4% - 50%。荟萃分析表明,接受手术和非手术治疗的患者在肝肿瘤负荷(比值比[OR]=1.51,95%置信区间:0.59 - 3.89,P = 0.39)或肿瘤分级(OR = 2.88,95%置信区间:0.92 - 9.04,P = 0.07)方面无显著差异。此外,接受积极手术治疗的患者似乎肿瘤分级更高。然而,荟萃分析表明,接受原发性肿瘤切除的患者总生存期更好(P<0.001),合并风险比为0.36(95%置信区间:0.30 - 0.45)。未检测到发表偏倚。
本荟萃分析表明,对于PNETs合并无法切除肝转移的患者,姑息性切除原发性肿瘤可提高生存率,尽管对于身体状况较好、疾病进展程度较低或肿瘤位于胰体或胰尾的患者,似乎更倾向于采用更积极的手术方式。需要进行随访期更长的RCT来证实PNETs姑息性原发性肿瘤切除的优势。