Huang Xi-Tai, Xie Jin-Zhao, Chen Liu-Hua, Cai Jian-Peng, Chen Wei, Liang Li-Jian, Zhang Ning, Yin Xiao-Yu
Department of Pancreato-Biliary Surgery, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, P. R. China.
Department of Gastroenterology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, P. R. China.
Gastroenterol Rep (Oxf). 2023 Mar 8;11:goad010. doi: 10.1093/gastro/goad010. eCollection 2023.
The value of debulking surgery for unresectable well-differentiated metastatic pancreatic neuroendocrine tumor (m-PNET) remains poorly defined. This study aimed to evaluate the outcomes of m-PNET following debulking surgery in our institute.
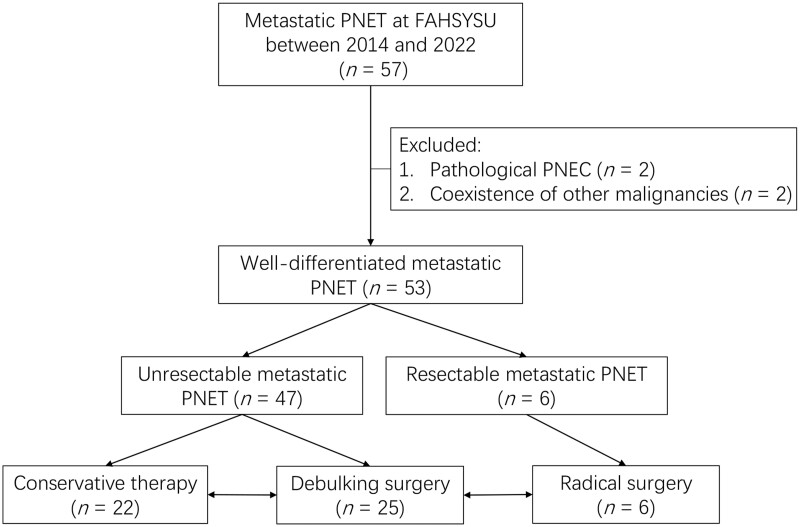
Patients with well-differentiated m-PNET in our hospital between February 2014 and March 2022 were collected. Clinicopathological and long-term outcomes of patients treated with radical resection, debulking surgery, and conservative therapy were compared retrospectively.
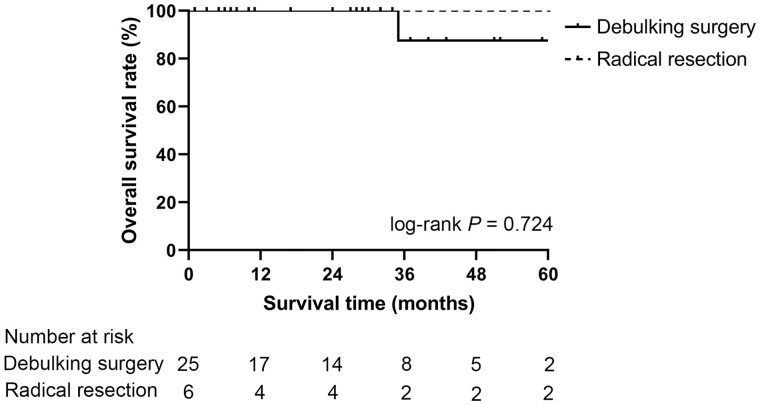
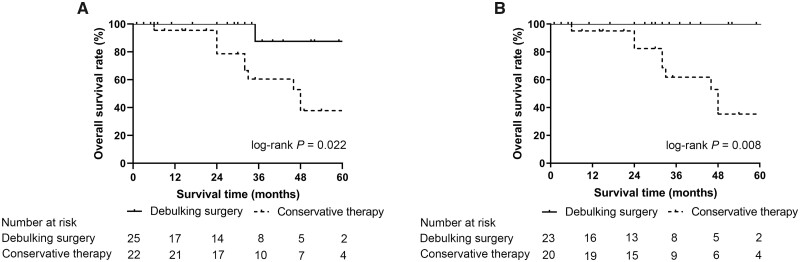
Fifty-three patients with well-differentiated m-PNET were reviewed, including 47 patients with unresectable m-PNET (debulking surgery, 25; conservative therapy, 22) and 6 patients with resectable m-PNET (radical resection). Patients undergoing debulking surgery had a post-operative Clavien-Dindo ≥ III complication rate of 16.0% without mortality. The 5-year overall survival (OS) rate of patients treated with debulking surgery was significantly higher than that of those treated with conservative therapy alone (87.5% vs 37.8%, log-rank =0.022). Besides, the 5-year OS rate of patients treated with debulking surgery was comparable to that of patients with resectable m-PNET undergoing radical resection (87.5% vs 100%, log-rank =0.724).
Patients with unresectable well-differentiated m-PNET who underwent resection had better long-term outcomes than those who received conservative therapy alone. The 5-year OS of patients undergoing debulking surgery and radical resection were comparable. Debulking surgery could be considered for patients with unresectable well-differentiated m-PNET if no contraindication exists.
减瘤手术对于无法切除的高分化转移性胰腺神经内分泌肿瘤(m-PNET)的价值仍未明确界定。本研究旨在评估我院行减瘤手术后m-PNET的治疗效果。
收集2014年2月至2022年3月期间我院收治的高分化m-PNET患者。对接受根治性切除、减瘤手术及保守治疗患者的临床病理特征及长期治疗效果进行回顾性比较。
共纳入53例高分化m-PNET患者,其中47例为无法切除的m-PNET(减瘤手术25例;保守治疗22例),6例为可切除的m-PNET(根治性切除)。接受减瘤手术的患者术后Clavien-Dindo≥Ⅲ级并发症发生率为16.0%,无死亡病例。接受减瘤手术患者的5年总生存率显著高于单纯接受保守治疗的患者(87.5%对37.8%,对数秩检验P=0.022)。此外,接受减瘤手术患者的5年总生存率与接受根治性切除的可切除m-PNET患者相当(87.5%对100%,对数秩检验P=0.724)。
无法切除的高分化m-PNET患者接受手术切除后的长期治疗效果优于单纯接受保守治疗的患者。减瘤手术和根治性切除患者的5年总生存率相当。对于无法切除的高分化m-PNET患者,若不存在禁忌证,可考虑行减瘤手术。