Williams Jelani K, Schwarz Jason L, Keutgen Xavier M
Division of General Surgery and Surgical Oncology, Department of Surgery, University of Chicago Medicine, Chicago, IL, USA.
Hepatobiliary Surg Nutr. 2023 Feb 28;12(1):69-83. doi: 10.21037/hbsn-22-238. Epub 2023 Jan 16.
Pancreatic neuroendocrine tumors (PanNETs) are derived from the islet cells of the pancreas and have been increasing in incidence. Most of these tumors are nonfunctional although some can secrete hormones and lead to hormone-specific clinical syndromes. Surgery is the mainstay of treatment for localized tumors, however, surgical resection is controversial in metastatic PanNETs. This narrative review seeks to summarize the current literature surrounding surgery, specifically in the controversial area of metastatic PanNETs, review current treatment paradigms, and understand the benefits of surgery in this group of patients.
Authors searched PubMed using the terms "surgery pancreatic neuroendocrine tumor", "metastatic neuroendocrine tumor", and "liver debulking neuroendocrine tumor" from January 1990 to June 2022. Only English language publications were considered.
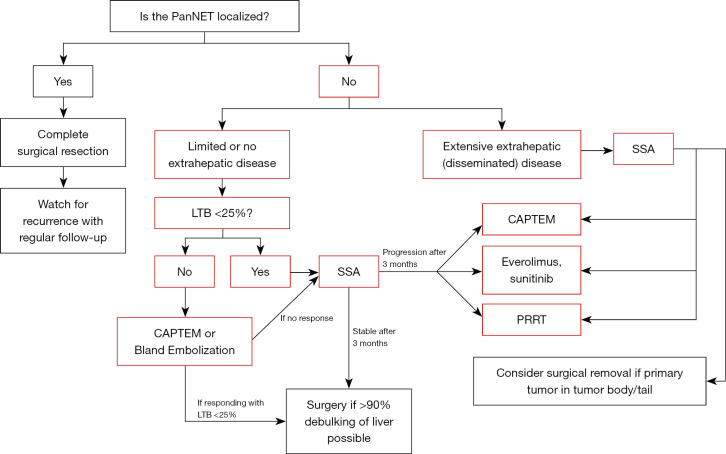
There is no consensus among the leading specialty organizations regarding surgery for metastatic PanNETs. When considering surgery for metastatic PanNETs, tumor grade and morphology, location of the primary tumor, extra-hepatic or extra-abdominal disease, as well as liver tumor burden and metastatic distribution should be considered. Because the liver is the most common site of metastasis and liver failure is the most common cause of death in patients with hepatic metastases, attention is centered here on debulking and other ablative techniques. Liver transplantation is rarely used for hepatic metastases but could be beneficial in a small subset of patients. Retrospective studies have demonstrated improvement in survival and symptoms after surgery for metastatic disease, but the lack of prospective randomized control trials significantly limits analysis of surgical benefits in patients with metastatic PanNETs.
Surgery is the standard of care for localized PanNETs, while it remains controversial in metastatic disease. Many studies have shown a survival and symptomatic benefit to surgery and liver debulking in select groups of patients. However, most of the studies on which recommendations are based in this population are retrospective in nature and are subject to selection bias. This presents an opportunity for future investigation.
胰腺神经内分泌肿瘤(PanNETs)起源于胰腺胰岛细胞,其发病率呈上升趋势。这些肿瘤大多无功能,不过有些可分泌激素并导致特定激素相关的临床综合征。手术是局限性肿瘤的主要治疗方法,然而,对于转移性PanNETs,手术切除存在争议。本叙述性综述旨在总结当前围绕手术的文献,特别是在转移性PanNETs这一有争议的领域,回顾当前的治疗模式,并了解手术对这类患者的益处。
作者于1990年1月至2022年6月期间在PubMed上使用“手术 胰腺神经内分泌肿瘤”“转移性神经内分泌肿瘤”和“肝脏减瘤神经内分泌肿瘤”等检索词进行搜索。仅纳入英文出版物。
主要专业组织对于转移性PanNETs的手术治疗尚无共识。在考虑对转移性PanNETs进行手术时,应考虑肿瘤分级和形态、原发肿瘤位置、肝外或腹外疾病,以及肝脏肿瘤负荷和转移分布情况。由于肝脏是最常见的转移部位,肝衰竭是肝转移患者最常见的死亡原因,因此这里将重点放在减瘤及其他消融技术上。肝移植很少用于肝转移,但可能对一小部分患者有益。回顾性研究表明,转移性疾病手术后生存率和症状有所改善,但缺乏前瞻性随机对照试验显著限制了对转移性PanNETs患者手术益处的分析。
手术是局限性PanNETs的标准治疗方法,而在转移性疾病中仍存在争议。许多研究表明,在特定患者群体中手术和肝脏减瘤可带来生存和症状改善。然而,该人群中大多数作为推荐依据的研究本质上是回顾性的,且存在选择偏倚。这为未来的研究提供了机会。