Azoulay Elie, Lemiale Virginie, Mokart Djamel, Nseir Saad, Argaud Laurent, Pène Frédéric, Kontar Loay, Bruneel Fabrice, Klouche Kada, Barbier François, Reignier Jean, Stoclin Anabelle, Louis Guillaume, Constantin Jean-Michel, Mayaux Julien, Wallet Florent, Kouatchet Achille, Peigne Vincent, Perez Pierre, Girault Christophe, Jaber Samir, Oziel Johanna, Nyunga Martine, Terzi Nicolas, Bouadma Lila, Lebert Christine, Lautrette Alexandre, Bigé Naike, Raphalen Jean-Herlé, Papazian Laurent, Rabbat Antoine, Darmon Michael, Chevret Sylvie, Demoule Alexandre
Medical Intensive Care Unit, APHP, Hôpital Saint-Louis. ECSTRA Team, and Clinical Epidemiology, UMR 1153, (Center of Epidemiology and Biostatistics, Sorbonne Paris Cité, CRESS), INSERM, Paris Diderot Sorbonne University, Paris, France.
Intensive Care Unit, Paoli Calmettes Institut, Marseille, France.
Trials. 2018 Mar 5;19(1):157. doi: 10.1186/s13063-018-2492-z.
Acute respiratory failure (ARF) is the leading reason for intensive care unit (ICU) admission in immunocompromised patients. High-flow nasal oxygen (HFNO) therapy is an alternative to standard oxygen. By providing warmed and humidified gas, HFNO allows the delivery of higher flow rates via nasal cannula devices, with FiO values of nearly 100%. Benefits include alleviation of dyspnea and discomfort, decreased respiratory distress and decreased mortality in unselected patients with acute hypoxemic respiratory failure. However, in preliminary reports, HFNO benefits are controversial in immunocompromised patients in whom it has never been properly evaluated.
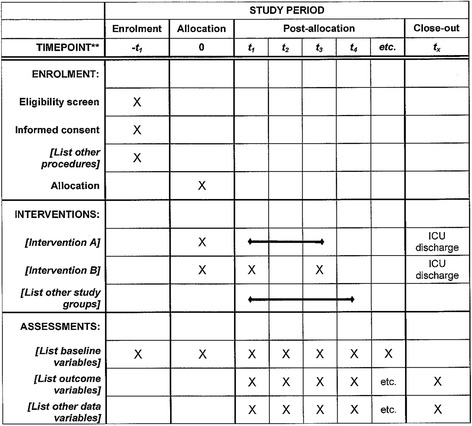
METHODS/DESIGN: This is a multicenter, open-label, randomized controlled superiority trial in 30 intensive care units, part of the Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique (GRRR-OH). Inclusion criteria will be: (1) adults, (2) known immunosuppression, (3) ARF, (4) oxygen therapy ≥ 6 L/min, (5) written informed consent from patient or proxy. Exclusion criteria will be: (1) imminent death (moribund patient), (2) no informed consent, (3) hypercapnia (PaCO ≥ 50 mmHg), (4) isolated cardiogenic pulmonary edema, (5) pregnancy or breastfeeding, (6) anatomical factors precluding insertion of a nasal cannula, (7) no coverage by the French statutory healthcare insurance system, and (8) post-surgical setting from day 1 to day 6 (patients with ARF occurring after day 6 of surgery can be included). The primary outcome measure is day-28 mortality. Secondary outcomes are intubation rate, comfort, dyspnea, respiratory rate, oxygenation, ICU length of stay, and ICU-acquired infections. Based on an expected 30% mortality rate in the standard oxygen group, and 20% in the HFNO group, error rate set at 5%, and a statistical power at 90%, 389 patients are required in each treatment group (778 patients overall). Recruitment period is estimated at 30 months, with 28 days of additional follow-up for the last included patient.
The HIGH study will be the largest multicenter, randomized controlled trial seeking to demonstrate that survival benefits from HFNO reported in unselected patients also apply to a large immunocompromised population.
ClinicalTrials.gov, ID: NCT02739451 . Registered on 15 April 2016.
急性呼吸衰竭(ARF)是免疫功能低下患者入住重症监护病房(ICU)的主要原因。高流量鼻导管吸氧(HFNO)疗法是标准氧疗的一种替代方法。通过提供温热、湿润的气体,HFNO能够经鼻导管装置输送更高的流速,吸氧浓度(FiO)值接近100%。其益处包括缓解呼吸困难和不适、减轻呼吸窘迫以及降低未选择的急性低氧性呼吸衰竭患者的死亡率。然而,在初步报告中,HFNO对免疫功能低下患者的益处存在争议,且从未得到过恰当评估。
方法/设计:这是一项在30个重症监护病房进行的多中心、开放标签、随机对照优势试验,是血液肿瘤重症监护呼吸研究组(GRRR-OH)的一部分。纳入标准为:(1)成年人;(2)已知免疫抑制;(3)ARF;(4)氧疗≥6升/分钟;(5)患者或代理人签署书面知情同意书。排除标准为:(1)濒死(垂死患者);(2)未签署知情同意书;(3)高碳酸血症(动脉血二氧化碳分压[PaCO]≥50 mmHg);(4)单纯心源性肺水肿;(5)妊娠或哺乳期;(6)存在妨碍插入鼻导管的解剖因素;(7)未纳入法国法定医疗保险系统覆盖范围;(8)术后第1天至第6天(术后第6天之后发生ARF的患者可纳入)。主要结局指标是第28天的死亡率。次要结局指标包括插管率、舒适度、呼吸困难、呼吸频率、氧合、ICU住院时间以及ICU获得性感染。基于标准氧疗组预期死亡率为30%,HFNO组为20%,设定错误率为5%,统计效能为90%,每个治疗组需要389例患者(总共778例患者)。预计招募期为30个月,对最后纳入的患者额外随访28天。
HIGH研究将是最大规模的多中心随机对照试验之一,旨在证明未选择患者中报告的HFNO生存获益也适用于大量免疫功能低下人群。
ClinicalTrials.gov,标识符:NCT02739451。于2016年4月15日注册。