Zhang Wei, De Debapriya, Mohammed Kahee A, Munigala Satish, Chen Guilan, Lai Jin-Ping, Bacon Bruce R
Department of Internal Medicine Saint Louis University School of Medicine St Louis MO.
Division of Gastroenterology and Hepatology Saint Louis University School of Medicine St Louis MO.
Hepatol Commun. 2018 Feb 20;2(3):245-253. doi: 10.1002/hep4.1148. eCollection 2018 Mar.
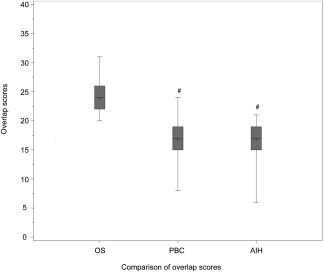
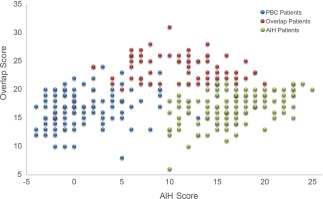
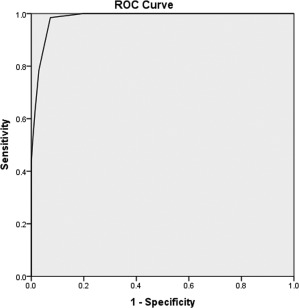
Autoimmune hepatitis (AIH) and primary biliary cholangitis (PBC) are two major immune-mediated chronic liver diseases. Overlap syndrome (OS) is diagnosed if patients have features of both AIH and PBC; however, there is no consensus on the definition or diagnostic criteria for OS. Here, we report a new scoring classification for OS and evaluate its usefulness. This new scoring classification was developed by modifying the International Autoimmune Hepatitis Group classification by selecting histologic features of AIH and PBC along with modifications of biochemical and immunologic characteristics. We evaluated 272 patients with chronic liver disease, including 105 with AIH, 102 with PBC, and 65 with OS. The best performance for the diagnosis of OS was noted among patients with an overlap score of ≥21 who had a sensitivity of 98.5%, a specificity of 92.8%, a positive predictive value of 81.0%, and a negative predictive value of 99.5%. By using a cut-off score of 21, 64 (98.5%) patients were diagnosed with OS as opposed to 9 (8.8%) and 6 (5.7%) with PBC and AIH, respectively. All patients with OS had an aggregate score of >19, whereas most patients with PBC or AIH scored <19, making this a safe discriminatory cut-off point against OS. : The new scoring system for the diagnosis of OS has a high sensitivity and specificity for scores ≥21, while a score <19 suggests a diagnosis other than OS. This classification can identify patients and diagnose OS with a reasonable amount of accuracy and may be superior to current OS scoring systems in detecting mild forms of OS. ( 2018;2:245-253).
自身免疫性肝炎(AIH)和原发性胆汁性胆管炎(PBC)是两种主要的免疫介导性慢性肝病。如果患者同时具有AIH和PBC的特征,则诊断为重叠综合征(OS);然而,对于OS的定义或诊断标准尚无共识。在此,我们报告一种针对OS的新评分分类方法并评估其效用。这种新的评分分类方法是通过修改国际自身免疫性肝炎小组的分类方法而制定的,具体做法是选择AIH和PBC的组织学特征,并对生化和免疫学特征进行修改。我们评估了272例慢性肝病患者,其中105例为AIH患者,102例为PBC患者,65例为OS患者。重叠评分≥21的患者对OS诊断的表现最佳,其灵敏度为98.5%,特异性为92.8%,阳性预测值为81.0%,阴性预测值为99.5%。使用21分的临界值时,64例(98.5%)患者被诊断为OS,相比之下,分别有9例(8.8%)和6例(5.7%)患者被诊断为PBC和AIH。所有OS患者的总分均>19,而大多数PBC或AIH患者的得分<19,这使其成为与OS进行安全区分的临界值。:用于诊断OS的新评分系统对≥21分的评分具有较高的灵敏度和特异性,而<19分的评分提示诊断不是OS。这种分类方法能够以合理的准确度识别患者并诊断OS,在检测轻度OS形式方面可能优于当前的OS评分系统。(2018;2:245 - 253)