Department of Clinical and Experimental Epilepsy, UCL Institute of Neurology, National Hospital for Neurology and Neurosurgery, London, UK.
Epilepsy Society MRI Unit, Chalfont St Peter, UK.
Epilepsia. 2018 Apr;59(4):814-824. doi: 10.1111/epi.14034. Epub 2018 Mar 12.
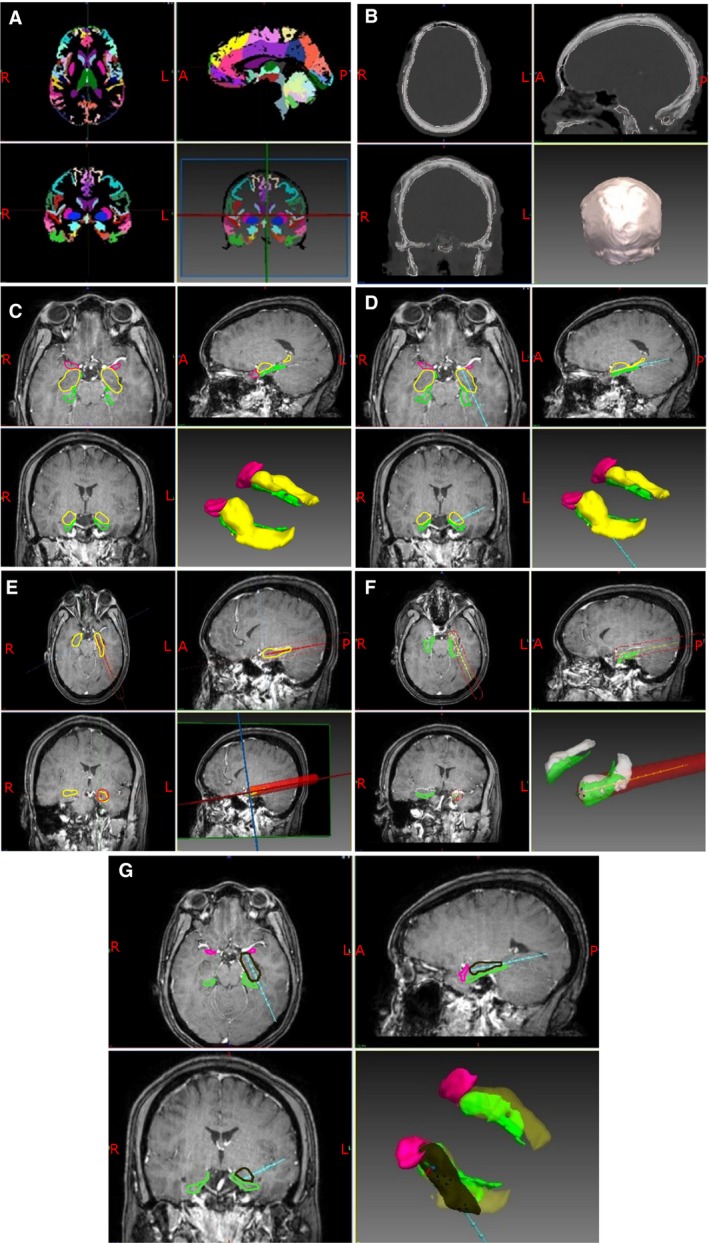
Surgical resection of the mesial temporal structures brings seizure remission in 65% of individuals with drug-resistant mesial temporal lobe epilepsy (MTLE). Laser interstitial thermal therapy (LiTT) is a novel therapy that may provide a minimally invasive means of ablating the mesial temporal structures with similar outcomes, while minimizing damage to the neocortex. Systematic trajectory planning helps ensure safety and optimal seizure freedom through adequate ablation of the amygdalohippocampal complex (AHC). Previous studies have highlighted the relationship between the residual unablated mesial hippocampal head and failure to achieve seizure freedom. We aim to implement computer-assisted planning (CAP) to improve the ablation volume and safety of LiTT trajectories.
Twenty-five patients who had previously undergone LiTT for MTLE were studied retrospectively. The EpiNav platform was used to automatically generate an optimal ablation trajectory, which was compared with the previous manually planned and implemented trajectory. Expected ablation volumes and safety profiles of each trajectory were modeled. The implemented laser trajectory and achieved ablation of mesial temporal lobe structures were quantified and correlated with seizure outcome.
CAP automatically generated feasible trajectories with reduced overall risk metrics (P < .001) and intracerebral length (P = .007). There was a significant correlation between the actual and retrospective CAP-anticipated ablation volumes, supporting a 15 mm diameter ablation zone model (P < .001). CAP trajectories would have provided significantly greater ablation of the amygdala (P = .0004) and AHC (P = .008), resulting in less residual unablated mesial hippocampal head (P = .001), and reduced ablation of the parahippocampal gyrus (P = .02).
Compared to manually planned trajectories CAP provides a better safety profile, with potentially improved seizure-free outcome and reduced neuropsychological deficits, following LiTT for MTLE.
手术切除内侧颞叶结构可使 65%的耐药性内侧颞叶癫痫(MTLE)患者癫痫发作缓解。激光间质热疗(LiTT)是一种新的治疗方法,它可以通过消融内侧颞叶结构提供一种微创的方法,同时最大限度地减少对新皮质的损伤。系统轨迹规划有助于通过充分消融杏仁核 - 海马复合体(AHC)来确保安全性和最佳的无癫痫发作。先前的研究强调了残留未消融的内侧海马头部与未能实现无癫痫发作之间的关系。我们旨在实施计算机辅助规划(CAP)以提高 LiTT 轨迹的消融体积和安全性。
回顾性研究了 25 例先前因 MTLE 而行 LiTT 的患者。使用 EpiNav 平台自动生成最佳消融轨迹,并将其与先前手动规划和实施的轨迹进行比较。对每条轨迹的预期消融体积和安全性特征进行建模。对实施的激光轨迹和实现的内侧颞叶结构消融进行量化,并与癫痫发作结果相关联。
CAP 自动生成的可行轨迹具有降低的总体风险指标(P <.001)和脑内长度(P =.007)。实际轨迹和回顾性 CAP 预测的消融体积之间存在显著相关性,支持 15 毫米直径消融区域模型(P <.001)。CAP 轨迹将提供明显更大的杏仁核(P =.0004)和 AHC 消融(P =.008),导致残留未消融的内侧海马头部更少(P =.001),以及减少对旁海马回的消融(P =.02)。
与手动规划的轨迹相比,CAP 提供了更好的安全性,在 LiTT 治疗 MTLE 后,可能具有更好的无癫痫发作结果和减少神经认知缺陷。