Vakharia Vejay N, Sparks Rachel, Rodionov Roman, Vos Sjoerd B, Dorfer Christian, Miller Jonathan, Nilsson Daniel, Tisdall Martin, Wolfsberger Stefan, McEvoy Andrew W, Miserocchi Anna, Winston Gavin P, O'Keeffe Aidan G, Ourselin Sebastien, Duncan John S
1Department of Clinical and Experimental Epilepsy, UCL Institute of Neurology, and.
2Epilepsy Society MRI Unit, Chalfont St Peter, United Kingdom.
J Neurosurg. 2018 Apr 13;130(2):601-610. doi: 10.3171/2017.10.JNS171826. Print 2018 Feb 1.
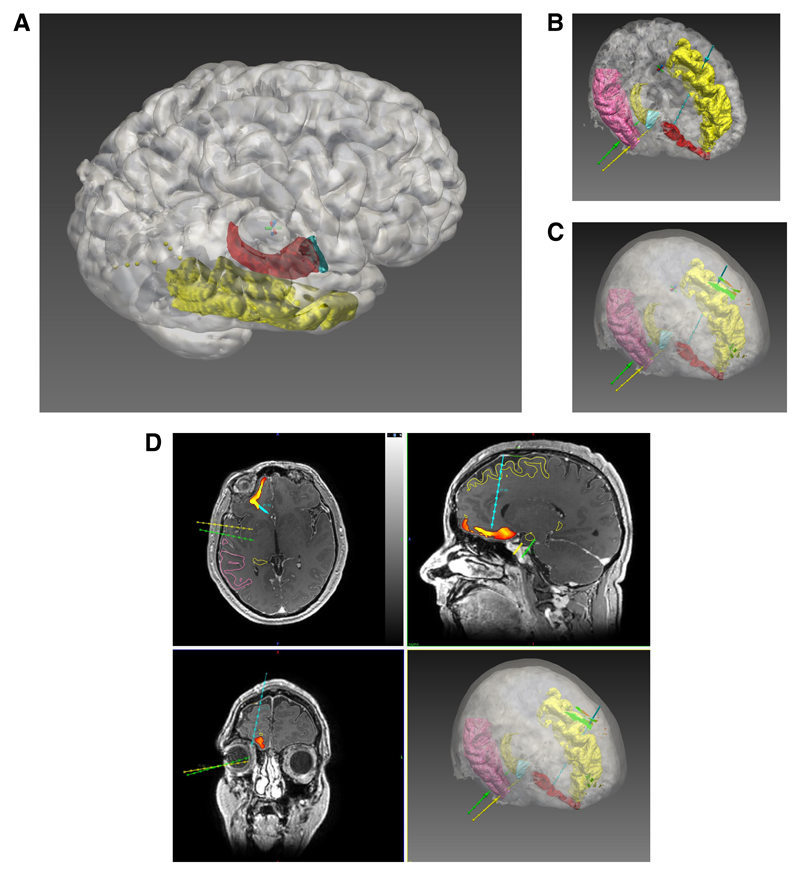
One-third of cases of focal epilepsy are drug refractory, and surgery might provide a cure. Seizure-free outcome after surgery depends on the correct identification and resection of the epileptogenic zone. In patients with no visible abnormality on MRI, or in cases in which presurgical evaluation yields discordant data, invasive stereoelectroencephalography (SEEG) recordings might be necessary. SEEG is a procedure in which multiple electrodes are placed stereotactically in key targets within the brain to record interictal and ictal electrophysiological activity. Correlating this activity with seizure semiology enables identification of the seizure-onset zone and key structures within the ictal network. The main risk related to electrode placement is hemorrhage, which occurs in 1% of patients who undergo the procedure. Planning safe electrode placement for SEEG requires meticulous adherence to the following: 1) maximize the distance from cerebral vasculature, 2) avoid crossing sulcal pial boundaries (sulci), 3) maximize gray matter sampling, 4) minimize electrode length, 5) drill at an angle orthogonal to the skull, and 6) avoid critical neurological structures. The authors provide a validation of surgical strategizing and planning with EpiNav, a multimodal platform that enables automated computer-assisted planning (CAP) for electrode placement with user-defined regions of interest.
Thirteen consecutive patients who underwent implantation of a total 116 electrodes over a 15-month period were studied retrospectively. Models of the cortex, gray matter, and sulci were generated from patient-specific whole-brain parcellation, and vascular segmentation was performed on the basis of preoperative MR venography. Then, the multidisciplinary implantation strategy and precise trajectory planning were reconstructed using CAP and compared with the implemented manually determined plans. Paired results for safety metric comparisons were available for 104 electrodes. External validity of the suitability and safety of electrode entry points, trajectories, and target-point feasibility was sought from 5 independent, blinded experts from outside institutions.
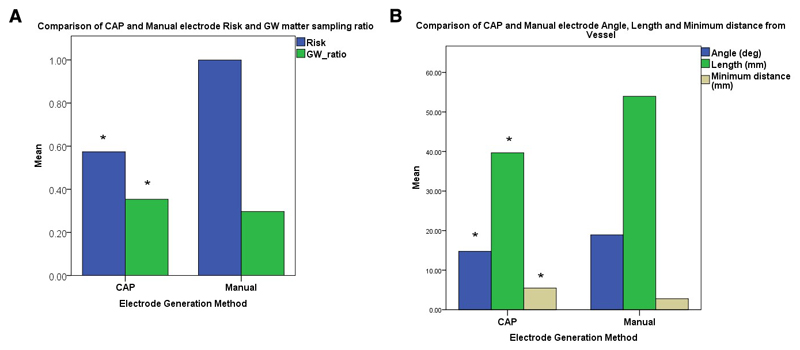
CAP-generated electrode trajectories resulted in a statistically significant improvement in electrode length, drilling angle, gray matter-sampling ratio, minimum distance from segmented vasculature, and risk (p < 0.05). The blinded external raters had various opinions of trajectory feasibility that were not statistically significant, and they considered a mean of 69.4% of manually determined trajectories and 62.2% of CAP-generated trajectories feasible; 19.4% of the CAP-generated electrode-placement plans were deemed feasible when the manually determined plans were not, whereas 26.5% of the manually determined electrode-placement plans were rated feasible when CAP-determined plans were not (no significant difference).
CAP generates clinically feasible electrode-placement plans and results in statistically improved safety metrics. CAP is a useful tool for automating the placement of electrodes for SEEG; however, it requires the operating surgeon to review the results before implantation, because only 62% of electrode-placement plans were rated feasible, compared with 69% of the manually determined placement plans, mainly because of proximity of the electrodes to unsegmented vasculature. Improved vascular segmentation and sulcal modeling could lead to further improvements in the feasibility of CAP-generated trajectories.
三分之一的局灶性癫痫病例药物难治,手术可能治愈。手术后无癫痫发作的结果取决于癫痫源区的正确识别和切除。对于磁共振成像(MRI)无明显异常的患者,或术前评估产生不一致数据的病例,可能需要进行侵入性立体定向脑电图(SEEG)记录。SEEG是一种将多个电极立体定向放置在脑内关键靶点以记录发作间期和发作期电生理活动的操作。将这种活动与癫痫发作症状学相关联,能够识别发作起始区和发作期网络内的关键结构。与电极放置相关的主要风险是出血,在接受该操作的患者中发生率为1%。为SEEG规划安全的电极放置需要严格遵循以下几点:1)最大化与脑血管的距离;2)避免穿过脑沟软脑膜边界(脑沟);3)最大化灰质采样;4)最小化电极长度;5)以与颅骨正交的角度钻孔;6)避免关键神经结构。作者使用EpiNav对手术策略制定和规划进行了验证,EpiNav是一个多模态平台,能够为电极放置进行自动计算机辅助规划(CAP),并带有用户定义的感兴趣区域。
回顾性研究了15个月内连续接受共116个电极植入的13例患者。从患者特异性全脑分割生成皮质、灰质和脑沟模型,并基于术前磁共振静脉造影进行血管分割。然后,使用CAP重建多学科植入策略和精确轨迹规划,并与实施的手动确定计划进行比较。104个电极有配对结果用于安全指标比较。从外部机构的5名独立、不知情的专家处寻求电极进入点、轨迹和靶点可行性的适用性和安全性的外部有效性评估。
CAP生成的电极轨迹在电极长度、钻孔角度、灰质采样率、与分割血管的最小距离和风险方面有统计学显著改善(p < 0.05)。不知情的外部评估者对轨迹可行性有不同意见,无统计学显著差异,他们认为手动确定轨迹中有69.4%可行,CAP生成轨迹中有62.2%可行;当手动确定的计划不可行时,CAP生成的电极放置计划中有19.4%被认为可行,而当CAP确定的计划不可行时,手动确定的电极放置计划中有26.5%被评为可行(无显著差异)。
CAP生成临床上可行的电极放置计划,并在统计学上改善了安全指标。CAP是用于自动进行SEEG电极放置的有用工具;然而,它要求手术医生在植入前审查结果,因为只有62%的电极放置计划被评为可行,而手动确定的放置计划为69%,主要原因是电极靠近未分割的血管。改进的血管分割和脑沟建模可能会进一步提高CAP生成轨迹的可行性。