Department of Clinical Laboratory, Jiangxi Province Key Laboratory of Laboratory Medicine, The Second Affiliated Hospital of Nanchang University, Nanchang, 330006, Jiangxi, China.
Cancer Med. 2018 Apr;7(4):1221-1231. doi: 10.1002/cam4.1428. Epub 2018 Mar 13.
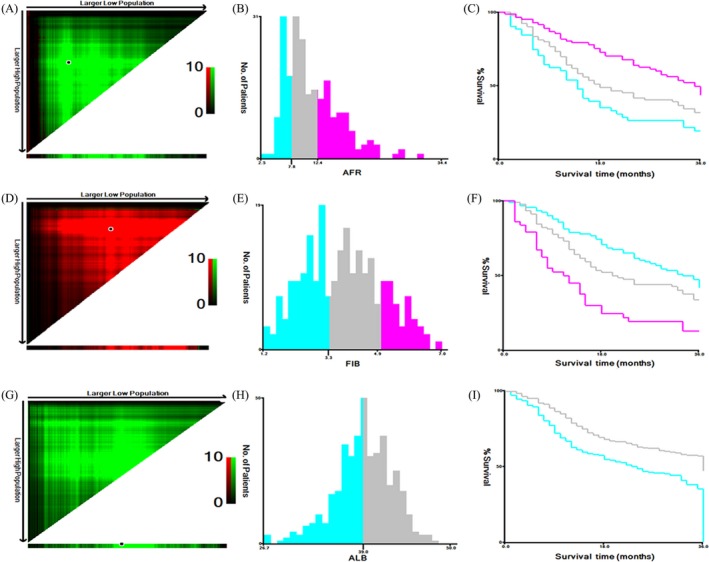
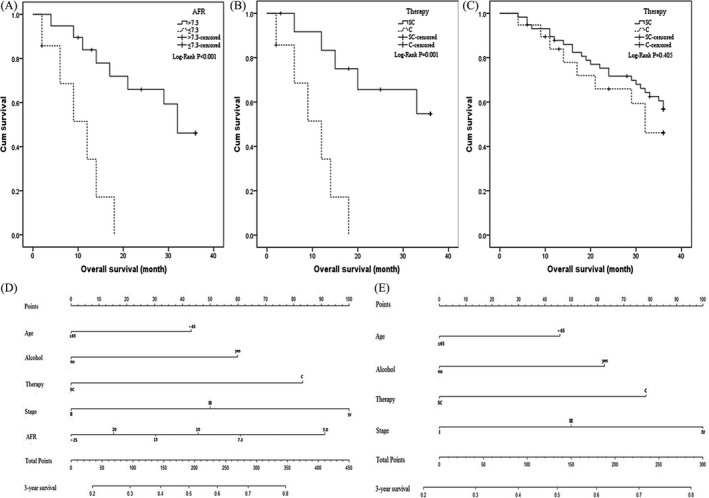
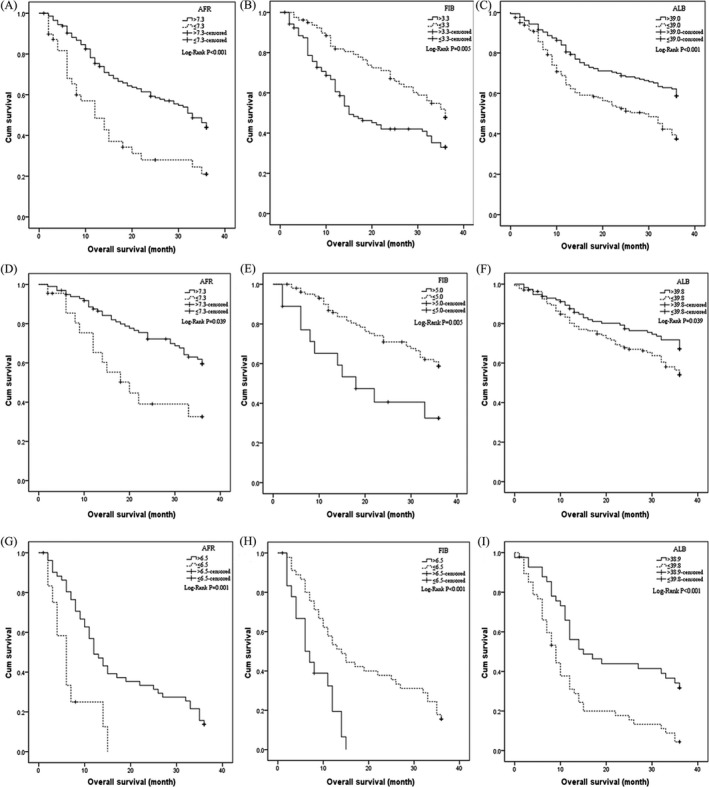
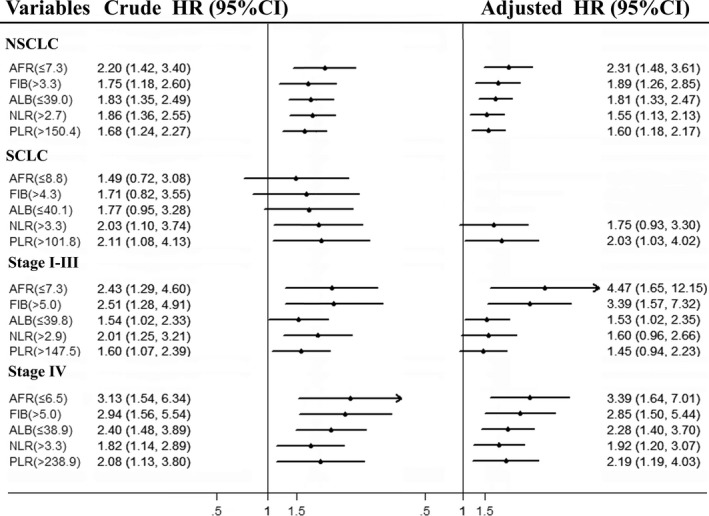
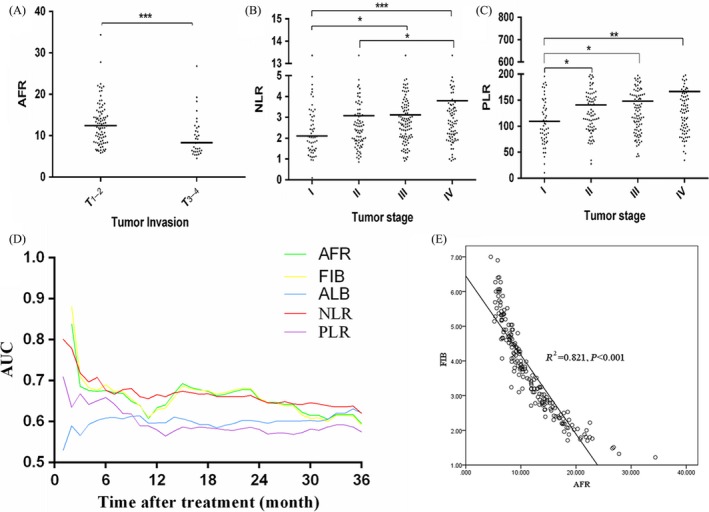
Chronic inflammation is one of the critical causes to promote the initiation and metastasis of solid malignancies including lung cancer (LC). Here, we aimed to investigate the prognostic roles of albumin (Alb)-to-fibrinogen (Fib) ratio (AFR), Fib and Alb in LC and to establish a novel effective nomogram combined with AFR. Four hundred twelve LC patients diagnosed between February 2005 and December 2014 were recruited in this prospective study. The prognostic roles of AFR, Fib, Alb, neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and monocyte-to-lymphocyte ratio (MLR) were identified by X-tile software, Kaplan-Meier curve, Cox regression model, and time-dependent ROC. Pretreatment high circulating Fib, low AFR, and Alb were significantly associated with increased risk of death for LC patients, especially for non-small cell lung cancer (NSCLC) patients in all stages. The area under curves (AUCs) of AFR, Fib, and NLR were higher than them within Alb and PLR for predicting the survival of NSCLC patients. Moreover, we found that clinical outcome of high AFR patient with chemo-radiotherapy was superior to low AFR patient; overall survival rate of stage II-III NSCLC patients undergoing chemo-radiotherapy was significantly lower than the surgical patients with treatment of adjuvant chemo-radiotherapy(P = 0.001) in low AFR subgroup. On the contrary, clinical outcome of the patients receiving chemo-radiotherapy was the same to the patients undergoing surgery and adjuvant chemo-radiotherapy (P = 0.405) in high AFR subgroup. In addition, c-index of predicted nomogram including AFR (0.717) for NSCLC patients with treatment of chemo-radiotherapy was higher than that without AFR (0.707). Our findings demonstrated that circulating pretreatment AFR might be a potential biomarker to predict clinical efficacy of surgical resection and adjuvant chemo-radiotherapy and be a prognostic biomarker for NSCLC individuals.
慢性炎症是促进包括肺癌(LC)在内的实体恶性肿瘤发生和转移的关键原因之一。在这里,我们旨在研究白蛋白(Alb)-纤维蛋白原(Fib)比值(AFR)、Fib 和 Alb 在 LC 中的预后作用,并建立一个结合 AFR 的新的有效列线图。本前瞻性研究纳入了 2005 年 2 月至 2014 年 12 月期间诊断的 412 例 LC 患者。使用 X-tile 软件、Kaplan-Meier 曲线、Cox 回归模型和时间依赖性 ROC 确定 AFR、Fib、Alb、中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)和单核细胞与淋巴细胞比值(MLR)的预后作用。术前高循环 Fib、低 AFR 和 Alb 与 LC 患者死亡风险增加显著相关,尤其是在所有分期的非小细胞肺癌(NSCLC)患者中。对于预测 NSCLC 患者的生存情况,AFR、Fib 和 NLR 的 AUC 均高于 Alb 和 PLR。此外,我们发现,接受放化疗的高 AFR 患者的临床结局优于低 AFR 患者;在低 AFR 亚组中,接受放化疗的 II-III 期 NSCLC 患者的总生存率明显低于接受手术治疗并接受辅助放化疗的患者(P=0.001)。相反,在高 AFR 亚组中,接受放化疗的患者的临床结局与接受手术和辅助放化疗的患者相同(P=0.405)。此外,接受放化疗的 NSCLC 患者预测列线图中包含 AFR 的 c-index(0.717)高于不包含 AFR 的 c-index(0.707)。我们的研究结果表明,术前循环 AFR 可能是预测手术切除和辅助放化疗临床疗效的潜在生物标志物,也是 NSCLC 患者的预后生物标志物。