Service d'Hématologie et Thérapie Cellulaire, Hôpital Saint Antoine, AP-HP, 168 Rue du Faubourg Saint Antoine, 75012, Paris, France.
Department of Pediatric Hematology and Oncology, IRCCS Bambino Gesù Children's Hospital, Piazza SOnofrio, 4, Roma, 00165, Italy.
J Hematol Oncol. 2018 Mar 15;11(1):40. doi: 10.1186/s13045-018-0586-4.
Experience using post-transplant cyclophosphamide (PT-Cy) as graft-versus-host disease (GVHD) prophylaxis in allogeneic stem cell transplantation (HSCT) from matched sibling donors (MSD) or unrelated donors (UD) is limited and with controversial results. The study aim was to evaluate PT-Cy as GVHD prophylaxis post-HSCT from MSD and UD transplants. We analyzed 423 patients with acute leukemia who received PT-Cy alone or in combination with other immunosuppressive (IS) drugs as GVHD prophylaxis. Seventy-eight patients received PT-Cy alone (group 1); 204 received PT-Cy in combination with one IS drug-cyclosporine-A (CSA) or methotrexate (MTX) or mycophenolate-mofetil (MMF) (group 2), while 141 patients received PT-Cy in combination with two IS drugs-CSA + MTX or CSA + MMF (group 3). Transplants were performed from 2007 to 2015 and median follow-up was 20 months.
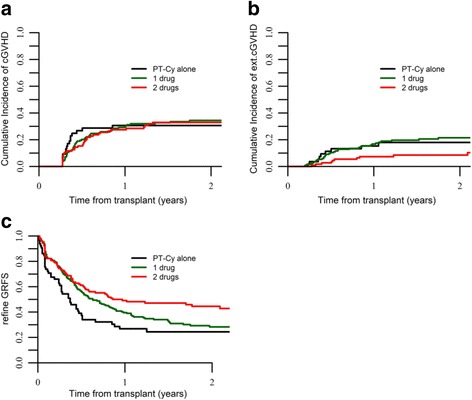
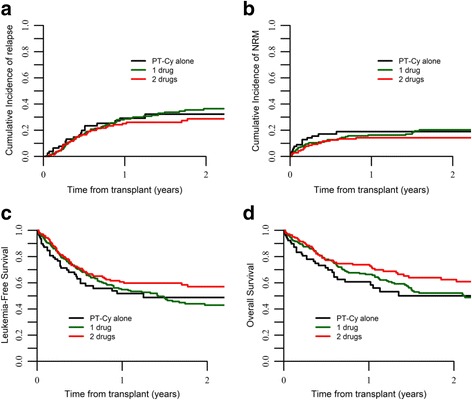
Probability of overall survival (OS) at 2 years was 50, 52.2, and 62.4%, for the three groups, respectively, p = 0.06. In multivariate analysis, in comparison to PT-Cy alone, the addition of two IS drugs was associated with reduced risk of extensive cGVHD (HR 0.25, p = 0.02). Use of bone marrow (BM) and anti-thymocyte globulin were independently associated with reduced risk of extensive cGVHD. Prognostic factors for non-relapse mortality (NRM) were the addition of two IS drugs to PT-Cy (HR 0.35, p = 0.04), diagnosis of AML, disease status at transplant, and patient CMV serology. Factors associated with increased OS were the use of PT-Cy with two IS drugs (HR 0.49, p = 0.02), AML, and disease status at transplant.
For GVHD prophylaxis in MSD and UD HSCT, the addition of IS drugs to PT-Cy enhances its effect and reduces the risk of severe cGVHD, reducing mortality and improving survival.
在异基因造血干细胞移植(HSCT)中,使用移植后环磷酰胺(PT-Cy)作为移植物抗宿主病(GVHD)预防的经验有限,且结果存在争议。本研究旨在评估来自匹配同胞供体(MSD)或无关供体(UD)的 HSCT 后使用 PT-Cy 作为 GVHD 预防的效果。我们分析了 423 例接受 PT-Cy 单独或与其他免疫抑制剂(IS)药物联合作为 GVHD 预防的急性白血病患者。78 例患者接受 PT-Cy 单独治疗(组 1);204 例患者接受 PT-Cy 联合一种 IS 药物-环孢素 A(CSA)或甲氨蝶呤(MTX)或霉酚酸酯(MMF)(组 2),而 141 例患者接受 PT-Cy 联合两种 IS 药物-CSA+MTX 或 CSA+MMF(组 3)。移植于 2007 年至 2015 年进行,中位随访时间为 20 个月。
三组患者的 2 年总生存(OS)概率分别为 50%、52.2%和 62.4%,p=0.06。多变量分析显示,与 PT-Cy 单独治疗相比,联合使用两种 IS 药物可降低广泛型慢性移植物抗宿主病(cGVHD)的风险(HR 0.25,p=0.02)。使用骨髓(BM)和抗胸腺细胞球蛋白与降低广泛型 cGVHD 的风险独立相关。非复发死亡率(NRM)的预后因素是将两种 IS 药物添加到 PT-Cy 中(HR 0.35,p=0.04)、诊断为急性髓系白血病(AML)、移植时疾病状态和患者巨细胞病毒血清学。与 OS 增加相关的因素是使用两种 IS 药物联合 PT-Cy(HR 0.49,p=0.02)、AML 和移植时疾病状态。
在 MSD 和 UD HSCT 中,将 IS 药物添加到 PT-Cy 中可增强其效果,降低严重 cGVHD 的风险,降低死亡率并改善生存。