Safai Narges, Carstensen Bendix, Vestergaard Henrik, Ridderstråle Martin
Patient Care, Steno Diabetes Center Copenhagen, Gentofte, Denmark.
Clinical Epidemiology, Steno Diabetes Center Copenhagen, Gentofte, Denmark.
BMJ Open. 2018 Mar 17;8(3):e019214. doi: 10.1136/bmjopen-2017-019214.
To investigate the impact of a multifactorial treatment programme in a real-life setting on clinical outcomes and estimated cardiovascular disease (CVD) risk.
A retrospective observational cohort study, using data from the electronic medical records and national registers.
Tertiary diabetes centre in Denmark.
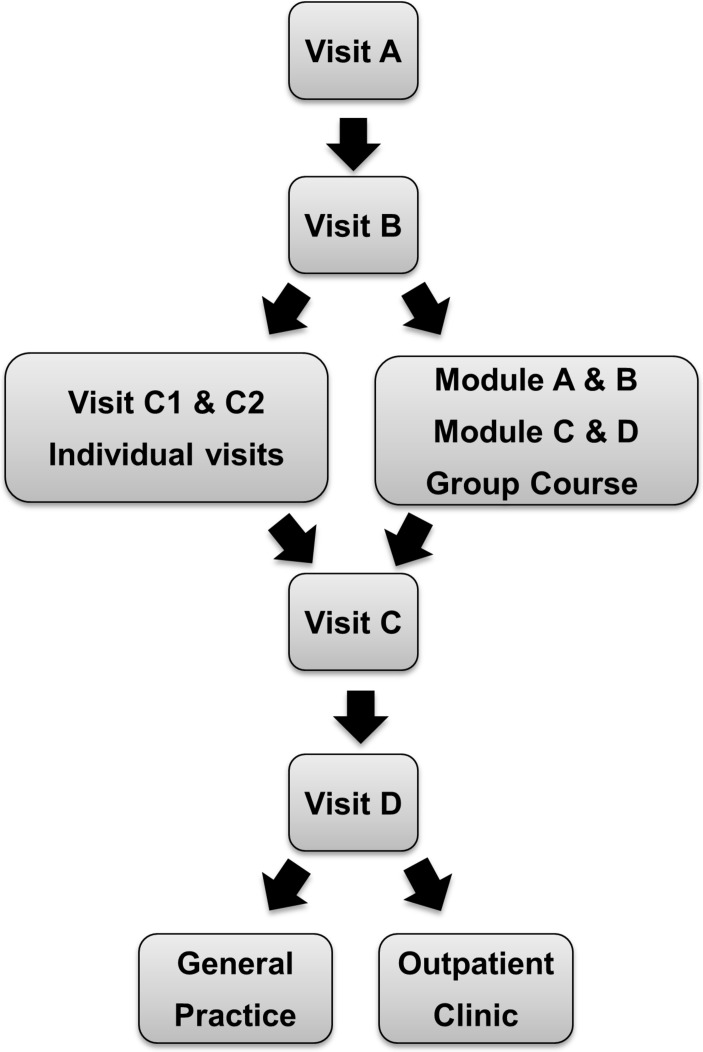
Patients with type 2 diabetes (n=4299) referred to a programme with focus on treatment of hyperglycaemia, hypertension and dyslipidaemia between 1 January 2001 and 1 April 2016.
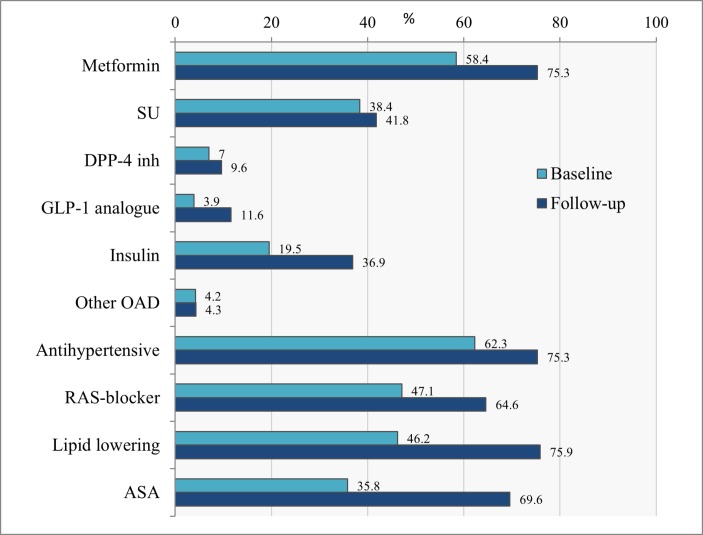
Primary outcomes were changes in haemoglobin A1c (HbA), blood pressure (BP) and low-density lipoprotein (LDL) cholesterol as well as proportion reaching treatment targets. Our secondary outcome was to investigate changes in antidiabetic, antihypertensive and lipid-lowering treatment, together with the impact on estimated CVD risk. Linear mixed model for repeated measurements were used for continuous variables and logistic regression for dichotomous variables.
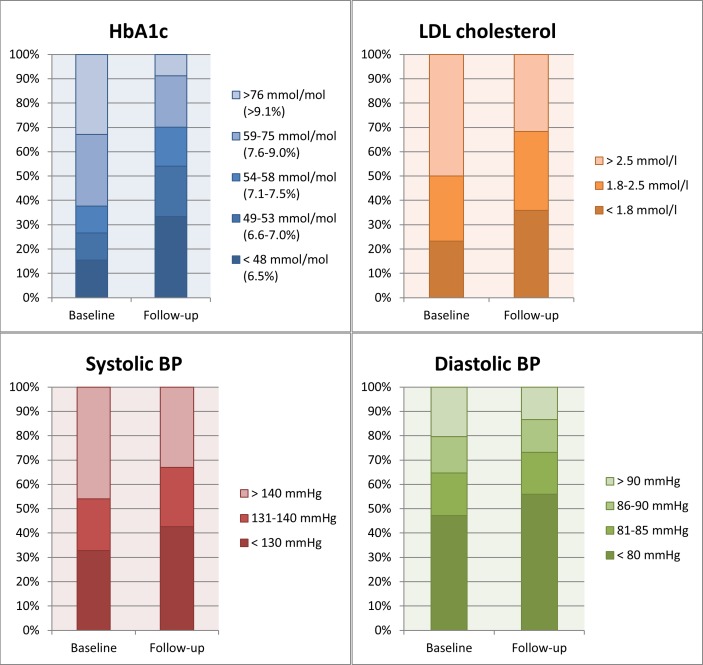
The patients achieved a mean±SD decrease in HbA, systolic and diastolic BP and LDL cholesterol of 1.0%±0.04% (10.6±0.4 mmol/mol), 6.3±0.4 mm Hg, 2.7±0.2 mm Hg and 0.32±0.02 mmol/L, respectively (p<0.0001). The proportion of patients who met the treatment goal for HbA (<7% (<53 mmol/mol)) increased from 31% to 58% (p<0.0001); for BP (<130/80 mm Hg) from 24% to 34% (p<0.0001), and for LDL cholesterol (<2.5 mmol/L (patients without previous CVD) or <1.8 mmol/L (patients with previous CVD)) from 52% to 65%. Those reaching all three guideline treatment targets increased from 4% to 15% (p<0.0001), and when relaxing the BP target to <140/85 from 8% to 24%. The estimated CVD risk was relatively reduced by 15.2% using the Swedish National Diabetes Register risk engine and 30.9% using the UK Prospective Diabetes Study risk engine.
Our data support that short-term multifactorial treatment of patients with glycaemic dysregulation in a specialist outpatient setting is both achievable and effective, and associated with a clinically meaningful improvement in CVD risk.
在实际生活环境中研究多因素治疗方案对临床结局和估计的心血管疾病(CVD)风险的影响。
一项回顾性观察性队列研究,使用电子病历和国家登记册中的数据。
丹麦的三级糖尿病中心。
2001年1月1日至2016年4月1日期间转诊至一个专注于高血糖、高血压和血脂异常治疗方案的2型糖尿病患者(n = 4299)。
主要结局为糖化血红蛋白(HbA)、血压(BP)和低密度脂蛋白(LDL)胆固醇的变化以及达到治疗目标的比例。我们的次要结局是研究抗糖尿病、抗高血压和降脂治疗的变化,以及对估计的CVD风险的影响。连续变量使用重复测量的线性混合模型,二分变量使用逻辑回归。
患者的HbA、收缩压和舒张压以及LDL胆固醇平均±标准差分别降低了1.0%±0.04%(10.6±0.4 mmol/mol)、6.3±0.4 mmHg、2.7±0.2 mmHg和0.32±0.02 mmol/L(p<0.0001)。达到HbA治疗目标(<7%(<53 mmol/mol))的患者比例从31%增至58%(p<0.0001);达到血压治疗目标(<130/80 mmHg)的患者比例从24%增至34%(p<0.0001),达到LDL胆固醇治疗目标(无既往CVD患者<2.5 mmol/L或有既往CVD患者<1.8 mmol/L)的患者比例从52%增至65%。达到所有三项指南治疗目标的患者比例从4%增至15%(p<0.0001),当将血压目标放宽至<140/85时,这一比例从8%增至24%。使用瑞典国家糖尿病登记风险引擎估计的CVD风险相对降低了15.2%,使用英国前瞻性糖尿病研究风险引擎估计的CVD风险相对降低了30.9%。
我们的数据支持在专科门诊环境中对血糖失调患者进行短期多因素治疗是可行且有效的,并且与CVD风险在临床上有意义的改善相关。