Section of Infectious Diseases and Immunity, Imperial College London, London, United Kingdom.
Front Immunol. 2018 Mar 2;9:323. doi: 10.3389/fimmu.2018.00323. eCollection 2018.
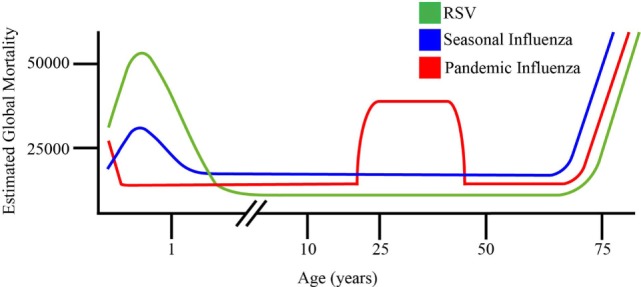
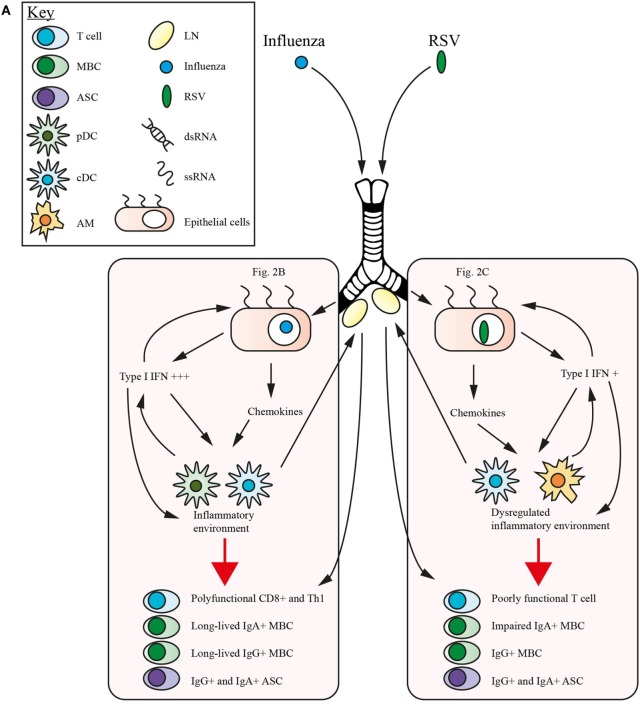
Respiratory syncytial virus (RSV) and influenza are among the most important causes of severe respiratory disease worldwide. Despite the clinical need, barriers to developing reliably effective vaccines against these viruses have remained firmly in place for decades. Overcoming these hurdles requires better understanding of human immunity and the strategies by which these pathogens evade it. Although superficially similar, the virology and host response to RSV and influenza are strikingly distinct. Influenza induces robust strain-specific immunity following natural infection, although protection by current vaccines is short-lived. In contrast, even strain-specific protection is incomplete after RSV and there are currently no licensed RSV vaccines. Although animal models have been critical for developing a fundamental understanding of antiviral immunity, extrapolating to human disease has been problematic. It is only with recent translational advances (such as controlled human infection models and high-dimensional technologies) that the mechanisms responsible for differences in protection against RSV compared to influenza have begun to be elucidated in the human context. Influenza infection elicits high-affinity IgA in the respiratory tract and virus-specific IgG, which correlates with protection. Long-lived influenza-specific T cells have also been shown to ameliorate disease. This robust immunity promotes rapid emergence of antigenic variants leading to immune escape. RSV differs markedly, as reinfection with similar strains occurs despite natural infection inducing high levels of antibody against conserved antigens. The immunomodulatory mechanisms of RSV are thus highly effective in inhibiting long-term protection, with disturbance of type I interferon signaling, antigen presentation and chemokine-induced inflammation possibly all contributing. These lead to widespread effects on adaptive immunity with impaired B cell memory and reduced T cell generation and functionality. Here, we discuss the differences in clinical outcome and immune response following influenza and RSV. Specifically, we focus on differences in their recognition by innate immunity; the strategies used by each virus to evade these early immune responses; and effects across the innate-adaptive interface that may prevent long-lived memory generation. Thus, by comparing these globally important pathogens, we highlight mechanisms by which optimal antiviral immunity may be better induced and discuss the potential for these insights to inform novel vaccines.
呼吸道合胞病毒 (RSV) 和流感是全球最重要的严重呼吸道疾病病因。尽管临床有需求,但几十年来,开发针对这些病毒的可靠有效疫苗的障碍仍然存在。克服这些障碍需要更好地了解人体免疫以及这些病原体逃避免疫的策略。尽管表面上相似,但 RSV 和流感的病毒学和宿主反应截然不同。流感在自然感染后会引发强大的株特异性免疫,尽管当前疫苗的保护作用是短暂的。相比之下,即使是 RSV 也无法实现完全的株特异性保护,目前也没有获得许可的 RSV 疫苗。尽管动物模型对于深入了解抗病毒免疫至关重要,但将其推广到人类疾病方面存在问题。只有随着最近的转化进展(如受控的人体感染模型和高维技术),才能开始在人类背景下阐明 RSV 与流感相比在保护方面存在差异的机制。流感感染会在呼吸道中引发高亲和力的 IgA 和病毒特异性 IgG,这与保护作用相关。已经证明,长寿的流感特异性 T 细胞也可以改善疾病。这种强大的免疫会促进抗原变异体的快速出现,从而导致免疫逃逸。RSV 则明显不同,因为即使在自然感染诱导针对保守抗原的高水平抗体后,仍会再次感染类似的株。因此,RSV 的免疫调节机制在抑制长期保护方面非常有效,可能涉及干扰 I 型干扰素信号传导、抗原呈递和趋化因子诱导的炎症等机制。这些机制会对适应性免疫产生广泛影响,导致 B 细胞记忆受损,T 细胞生成和功能降低。在这里,我们讨论了流感和 RSV 后临床结果和免疫反应的差异。具体来说,我们专注于它们在先天免疫识别方面的差异;每种病毒逃避这些早期免疫反应的策略;以及可能阻止长期记忆生成的固有-适应性界面的影响。因此,通过比较这些全球重要的病原体,我们强调了更好地诱导最佳抗病毒免疫的机制,并讨论了这些见解为新型疫苗提供信息的潜力。