Department of Veterans Affairs Salt Lake City Health Care System, Salt Lake City, UT, USA.
Veterans Health Administration, 200 Springs Road, Building 70, Bedford, MA, 01730, USA.
BMC Cancer. 2018 Mar 20;18(1):306. doi: 10.1186/s12885-018-4190-3.
Tumor testing for mutations in the epidermal growth factor receptor (EGFR) gene is indicated for all newly diagnosed, metastatic lung cancer patients, who may be candidates for first-line treatment with an EGFR tyrosine kinase inhibitor. Few studies have analyzed population-level testing.
We identified clinical, demographic, and regional predictors of EGFR & KRAS testing among Medicare beneficiaries with a new diagnosis of lung cancer in 2011-2013 claims. The outcome variable was whether the patient underwent molecular, EGFR and KRAS testing. Independent variables included: patient demographics, Medicaid status, clinical characteristics, and region where the patient lived. We performed multivariate logistic regression to identify factors that predicted testing.
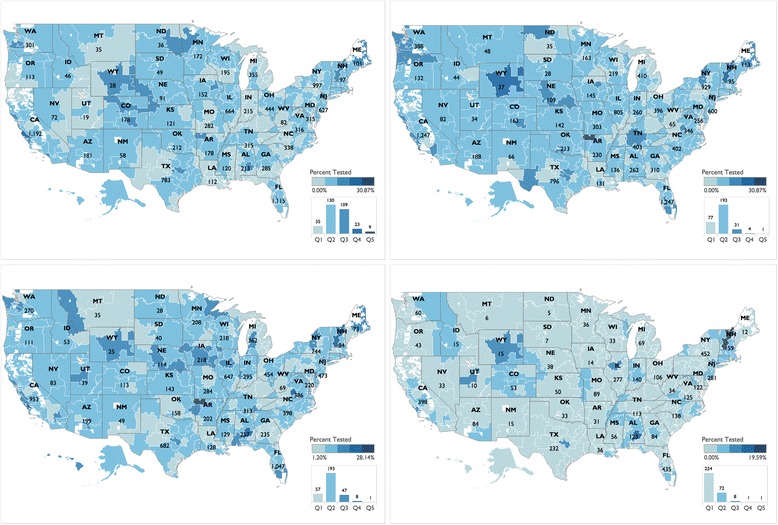
From 2011 to 2013, there was a 19.7% increase in the rate of EGFR testing. Patient zip code had the greatest impact on odds to undergo testing; for example, patients who lived in the Boston, Massachusetts hospital referral region were the most likely to be tested (odds ratio (OR) of 4.94, with a 95% confidence interval (CI) of 1.67-14.62). Patient demographics also impacted odds to be tested. Asian/Pacific Islanders were most likely to be tested (OR 1.63, CI 1.53-1.79). Minorities and Medicaid patients were less likely to be tested. Medicaid recipients had an OR of 0.74 (CI 0.72-0.77). Hispanics and Blacks were also less likely to be tested (OR 0.97, CI 0.78-0.99 and 0.95, CI 0.92-0.99), respectively. Clinical procedures were also correlated with testing. Patients who underwent transcatheter biopsies were 2.54 times more likely to be tested (CI 2.49-2.60) than those who did not undergo this type of biopsy.
Despite an overall increase in EGFR testing, there is widespread underutilization of guideline-recommended testing. We observed racial, income, and regional disparities in testing. Precision medicine has increased the complexity of cancer diagnosis and treatment. Targeted interventions and clinical decision support tools are needed to ensure that all patients are benefitting from advances in precision medicine. Without such interventions, precision medicine may exacerbate racial disparities in cancer care and health outcomes.
表皮生长因子受体(EGFR)基因突变的肿瘤检测适用于所有新诊断的转移性肺癌患者,这些患者可能是一线接受 EGFR 酪氨酸激酶抑制剂治疗的候选者。很少有研究分析人群水平的检测。
我们在 2011-2013 年的医疗保险索赔中确定了临床、人口统计学和区域因素,这些因素与新诊断为肺癌的医疗保险受益人的 EGFR 和 KRAS 检测有关。因变量是患者是否接受了分子、EGFR 和 KRAS 检测。自变量包括:患者的人口统计学特征、医疗补助状况、临床特征和患者居住的地区。我们进行了多变量逻辑回归分析,以确定预测检测的因素。
从 2011 年到 2013 年,EGFR 检测率增加了 19.7%。患者邮政编码对接受检测的几率影响最大;例如,居住在马萨诸塞州波士顿医院转诊区的患者最有可能接受检测(优势比(OR)为 4.94,95%置信区间(CI)为 1.67-14.62)。患者的人口统计学特征也影响了接受检测的几率。亚裔/太平洋岛民最有可能接受检测(OR 1.63,CI 1.53-1.79)。少数民族和医疗补助患者接受检测的可能性较小。医疗补助受助人的 OR 为 0.74(CI 0.72-0.77)。西班牙裔和非裔美国人也不太可能接受检测(OR 0.97,CI 0.78-0.99 和 0.95,CI 0.92-0.99)。临床程序也与检测相关。接受经导管活检的患者接受检测的可能性是未接受这种类型活检的患者的 2.54 倍(CI 2.49-2.60)。
尽管 EGFR 检测总体上有所增加,但指南推荐的检测仍未得到广泛应用。我们观察到检测方面存在种族、收入和地区差异。精准医学增加了癌症诊断和治疗的复杂性。需要有针对性的干预措施和临床决策支持工具,以确保所有患者都能从精准医学的进步中受益。如果没有这些干预措施,精准医学可能会加剧癌症护理和健康结果方面的种族差异。