Markey Cancer Center, University of Kentucky, Lexington, Kentucky, United States of America.
Division of Cancer Biostatistics, University of Kentucky, Lexington, Kentucky, United States of America.
PLoS One. 2020 Aug 18;15(8):e0237790. doi: 10.1371/journal.pone.0237790. eCollection 2020.
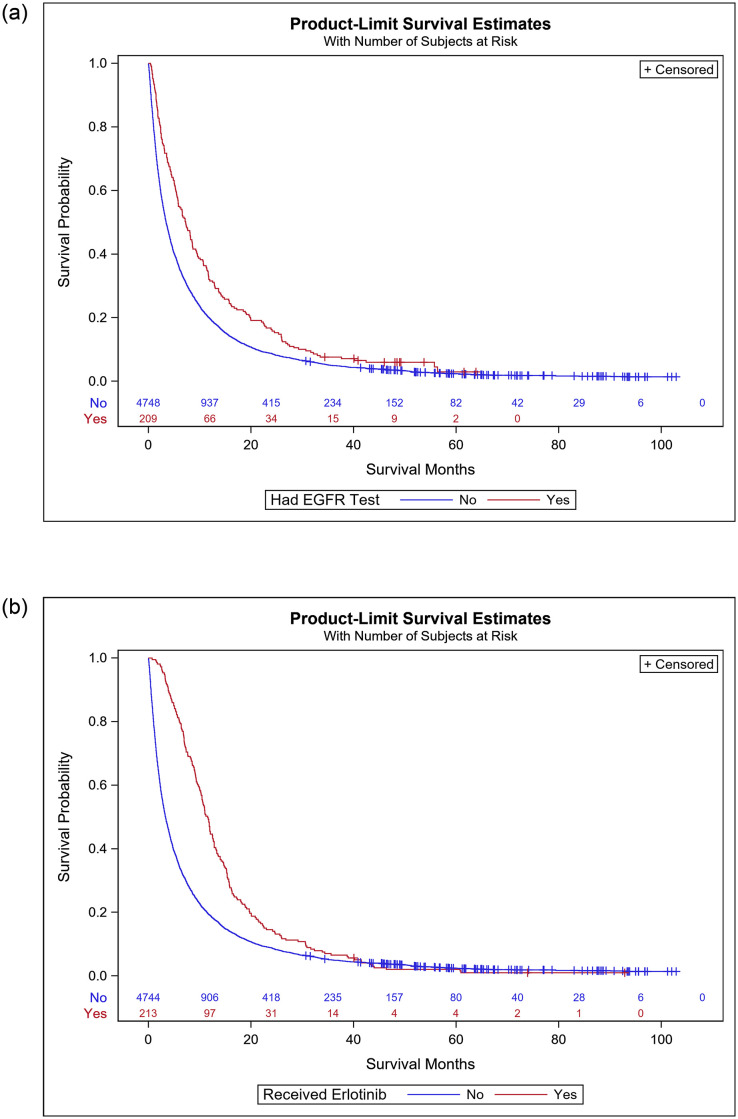
This study determined the frequency and factors associated with EGFR testing rates and erlotinib treatment as well as associated survival outcomes in patients with non small cell lung cancer in Kentucky. Data from the Kentucky Cancer Registry (KCR) linked with health claims from Medicaid, Medicare and private insurance groups were evaluated. EGFR testing and erlotinib prescribing were identified using ICD-9 procedure codes and national drug codes in claims, respectively. Logistic regression analysis was performed to determine factors associated with EGFR testing and erlotinib prescribing. Cox-regression analysis was performed to determine factors associated with survival. EGFR mutation testing rates rose from 0.1% to 10.6% over the evaluated period while erlotinib use ranged from 3.4% to 5.4%. Factors associated with no EGFR testing were older age, male gender, enrollment in Medicaid or Medicare, smoking, and geographic region. Factors associated with not receiving erlotinib included older age, male gender, enrollment in Medicare or Medicaid, and living in moderate to high poverty. Survival analysis demonstrated EGFR testing or erlotinib use was associated with a higher likelihood of survival. EGFR testing and erlotinib prescribing were slow to be implemented in our predominantly rural state. While population-level factors likely contributed, patient factors, including geographic location (areas with high poverty rates and rural regions) and insurance type, were associated with lack of use, highlighting rural disparities in the implementation of cancer precision medicine.
本研究旨在确定肯塔基州非小细胞肺癌患者中表皮生长因子受体(EGFR)检测率和厄洛替尼治疗率以及相关生存结果的频率和相关因素。肯塔基州癌症登记处(KCR)的数据与医疗补助、医疗保险和私人保险团体的健康索赔相关联,并进行评估。EGFR 检测和厄洛替尼处方是通过索赔中的 ICD-9 程序代码和国家药物代码确定的。采用逻辑回归分析确定与 EGFR 检测和厄洛替尼处方相关的因素。采用 Cox 回归分析确定与生存相关的因素。在评估期间,EGFR 突变检测率从 0.1%上升到 10.6%,而厄洛替尼的使用范围从 3.4%上升到 5.4%。与未进行 EGFR 检测相关的因素包括年龄较大、男性、参加医疗补助或医疗保险、吸烟和地理位置。与未接受厄洛替尼治疗相关的因素包括年龄较大、男性、参加医疗保险或医疗补助,以及居住在中高贫困地区。生存分析表明,EGFR 检测或厄洛替尼的使用与更高的生存可能性相关。在我们这个以农村为主的州,EGFR 检测和厄洛替尼的应用实施缓慢。尽管人口因素可能起到了作用,但患者因素,包括地理位置(高贫困率和农村地区)和保险类型,与未使用相关,突出了癌症精准医学实施中的农村差异。