Lauder Lucas, Ewen Sebastian, Tzafriri Abraham R, Edelman Elazer R, Cremers Bodo, Kulenthiran Saarraaken, Ukena Christian, Linz Dominik, Kindermann Ingrid, Tsioufis Costas, Scheller Bruno, Böhm Michael, Mahfoud Felix
Klinik für Innere Medizin III, Kardiologie, Angiologie und Internistische Intensivmedizin, Universitätsklinikum des Saarlandes, Universität des Saarlandes, Homburg, Saar, Germany.
Klinik für Innere Medizin III, Kardiologie, Angiologie und Internistische Intensivmedizin, Universitätsklinikum des Saarlandes, Universität des Saarlandes, Homburg, Saar, Germany.
Cardiovasc Revasc Med. 2018 Oct-Nov;19(7 Pt B):845-851. doi: 10.1016/j.carrev.2018.02.016. Epub 2018 Mar 2.
BACKGROUND/PURPOSE: Catheter-based renal sympathetic denervation (RDN) has been introduced to lower blood pressure (BP) and sympathetic activity in patients with uncontrolled hypertension with at best equivocal results. It has been postulated that anatomic and procedural elements introduce unaccounted variability and yet little is known of the impact of renal anatomy and procedural parameters on BP response to RDN.
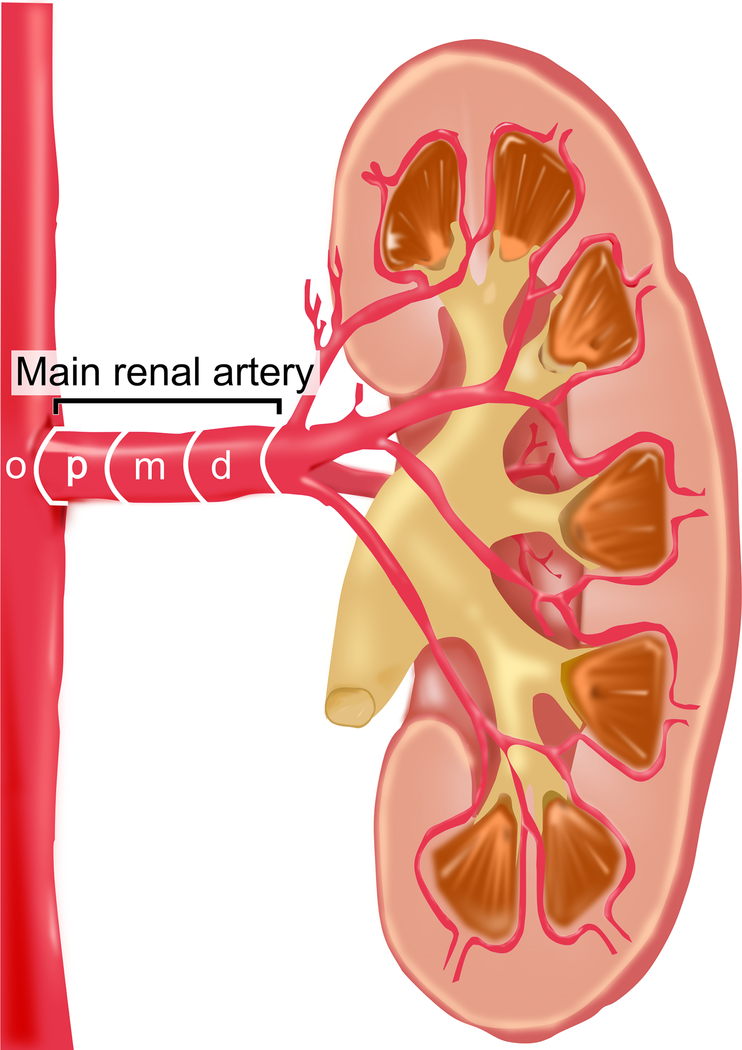
METHODS/MATERIALS: Anatomical parameters such as length and diameter were analyzed by quantitative vascular analysis and the prevalence of accessory renal arteries and renal artery disease were documented in 150 patients with resistant hypertension undergoing bilateral RDN using a mono-electrode radiofrequency catheter (Symplicity Flex, Medtronic).
Accessory renal arteries and renal artery disease were present in 56 (37%) and 14 patients (9%), respectively. At 6-months, 24 h-ambulatory BP was reduced by 11/6 mm Hg (p < 0.001 for both). Change of systolic blood pressure (SBP) was not related to the presence of accessory renal arteries (p = 0.543) or renal artery disease (p = 0.598). Patients with at least one main renal artery diameter ≤ 4 mm had a more pronounced reduction of 24 h-ambulatory SBP compared to patients where both arteries were >4 mm (-19 vs. -10 mmHg; p = 0.038). Neither the length of the renal artery nor the number of RF ablations influenced 24 h-ambulatory BP reduction at 6 months.
24 h-ambulatory BP lowering was most pronounced in patients with smaller renal artery diameter but not related to renal artery length, accessory arteries or renal artery disease. Further, there was no dose-response relationship observed with increasing number of ablations.
Because little is known of the impact of renal anatomy and procedural parameters on blood pressure (BP) response to renal denervation (RDN), anatomical and procedural data were analyzed in 150 patients undergoing bilateral RDN. BP lowering was most pronounced in patients with smaller renal artery diameter but not related to renal artery length, the presence of renal artery disease or accessory renal arteries. Further, there was no dose-response relationship observed with increasing number of ablations.
背景/目的:基于导管的肾交感神经去神经术(RDN)已被用于降低血压(BP)和交感神经活性,用于治疗难治性高血压患者,但结果充其量模棱两可。据推测,解剖学和操作因素会引入无法解释的变异性,然而,关于肾脏解剖结构和操作参数对RDN血压反应的影响知之甚少。
方法/材料:通过定量血管分析对长度和直径等解剖学参数进行分析,并记录了150例使用单电极射频导管(Symplicity Flex,美敦力公司)进行双侧RDN的难治性高血压患者的副肾动脉和肾动脉疾病的患病率。
分别有56例(37%)和14例(9%)患者存在副肾动脉和肾动脉疾病。6个月时,24小时动态血压降低了11/6 mmHg(两者p均<0.001)。收缩压(SBP)的变化与副肾动脉的存在(p = 0.543)或肾动脉疾病(p = 0.598)无关。至少有一条主肾动脉直径≤4 mm的患者,其24小时动态SBP的降低比两条动脉直径均>4 mm的患者更明显(-19 vs. -10 mmHg;p = 0.038)。肾动脉长度和射频消融次数均未影响6个月时24小时动态血压的降低。
肾动脉直径较小的患者24小时动态血压降低最为明显,但与肾动脉长度、副肾动脉或肾动脉疾病无关。此外,未观察到随着消融次数增加的剂量反应关系。
由于对肾脏解剖结构和操作参数对肾去神经术(RDN)血压反应的影响知之甚少,因此对150例接受双侧RDN的患者的解剖学和操作数据进行了分析。肾动脉直径较小的患者血压降低最为明显,但与肾动脉长度、肾动脉疾病或副肾动脉的存在无关。此外,未观察到随着消融次数增加的剂量反应关系。