Nagai Takashi, Naiki Taku, Iida Keitaro, Etani Toshiki, Ando Ryosuke, Hamamoto Shuzo, Sugiyama Yosuke, Akita Hidetoshi, Kubota Hiroki, Hashimoto Yoshihiro, Kawai Noriyasu, Yasui Takahiro
Department of Nephro-Urology, Nagoya City University, Graduate School of Medical Sciences, Nagoya, Japan.
Department of Urology, Anjo Kosei Hospital, Anjo City, Aichi Prefecture, Japan.
Prostate Int. 2018 Mar;6(1):18-23. doi: 10.1016/j.prnil.2017.07.001. Epub 2017 Aug 9.
Development of novel agents targeting the androgen axis has led to improved overall survival in castration-resistant prostate cancer (CRPC). This study aimed to investigate the optimal timing of treatment with one such agent, abiraterone acetate (AA), in Japanese patients.
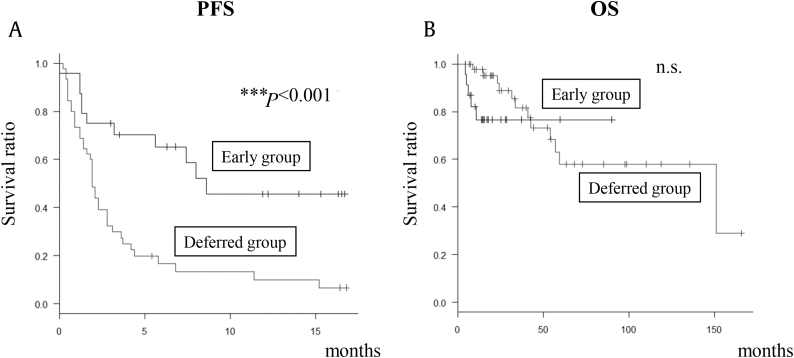
Between July 2014 and February 2016, 106 CRPC patients were administered AA in Nagoya City University Hospital, Nagoya, Japan and in four affiliated hospitals following failure of primary combined androgen blockade (CAB). Of these, records of 69 patients treated before chemotherapy were retrospectively analyzed. Patients were divided into two AA treatment groups: (1) first- or second-line after diagnosis of CRPC, designated the Early Group, and (2) third-line onwards, designated the Deferred Group. Prostate-specific antigen (PSA) response rate, ≥ 50% PSA decline rate with treatment, progression-free survival (PFS), and overall survival (OS) were compared between the two groups. National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0 was used to classify adverse events.
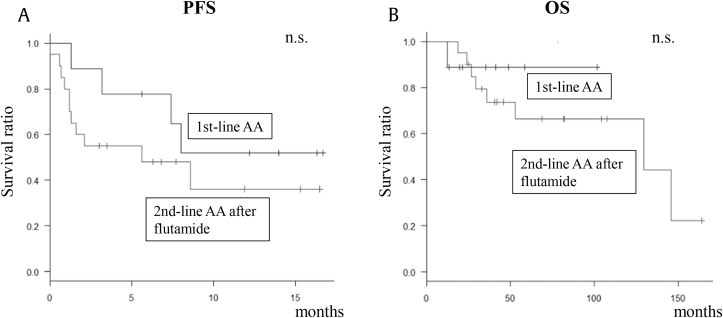
In 24 patients in the Early Group and 45 patients in the Deferred Group, no significant differences in baseline parameters were observed between groups. PSA response rate, ≥ 50% PSA decline rate and PFS (but not OS) were significantly better in the Early Group than in the Deferred Group. Serum aspartate aminotransferase/alanine aminotransferase elevations were the most common Grade 3 treatment-related toxicities, and were clinically manageable. In subgroup analyses of the Early Group, comparison of first-line AA with second-line AA after flutamide treatment showed no changes in PSA response rate, PFS, or OS.
This study suggests improved favorable outcomes of first- or second-line AA treatment in Japanese chemotherapy-naïve CRPC patients after failed CAB; statistical confirmation of such improvement was evident for PFS, but not OS. In addition, early AA treatment exhibited an acceptable safety profile.
针对雄激素轴的新型药物的研发已使去势抵抗性前列腺癌(CRPC)患者的总生存期得到改善。本研究旨在探讨在日本患者中使用其中一种药物醋酸阿比特龙(AA)进行治疗的最佳时机。
2014年7月至2016年2月期间,日本名古屋市立大学医院及四家附属医院对106例CRPC患者在一线联合雄激素阻断(CAB)治疗失败后给予AA治疗。其中,对69例化疗前接受治疗的患者记录进行回顾性分析。患者被分为两个AA治疗组:(1)CRPC诊断后的一线或二线治疗,指定为早期组;(2)三线及以后治疗,指定为延迟组。比较两组之间的前列腺特异性抗原(PSA)反应率、治疗后PSA下降率≥50%、无进展生存期(PFS)和总生存期(OS)。采用美国国立癌症研究所不良事件通用术语标准第4.0版对不良事件进行分类。
早期组24例患者和延迟组45例患者之间,各基线参数未观察到显著差异。早期组的PSA反应率、PSA下降率≥50%及PFS(但不包括OS)显著优于延迟组。血清天冬氨酸氨基转移酶/丙氨酸氨基转移酶升高是最常见的3级治疗相关毒性,且在临床上可控制。在早期组的亚组分析中,一线AA与氟他胺治疗后的二线AA比较,PSA反应率、PFS或OS无变化。
本研究提示,在日本初治CRPC患者CAB治疗失败后,一线或二线AA治疗有更好的有利结局;PFS有明显的统计学改善,但OS没有。此外,早期AA治疗具有可接受的安全性。