Department of Medicine, Northwestern University, Chicago, Illinois, United States of America.
University Medical Center Utrecht, Department of Vascular Medicine, Utrecht, Netherlands.
PLoS Med. 2018 Mar 20;15(3):e1002538. doi: 10.1371/journal.pmed.1002538. eCollection 2018 Mar.
Clinical practice guidelines have traditionally recommended blood pressure treatment based primarily on blood pressure thresholds. In contrast, using predicted cardiovascular risk has been advocated as a more effective strategy to guide treatment decisions for cardiovascular disease (CVD) prevention. We aimed to compare outcomes from a blood pressure-lowering treatment strategy based on predicted cardiovascular risk with one based on systolic blood pressure (SBP) level.
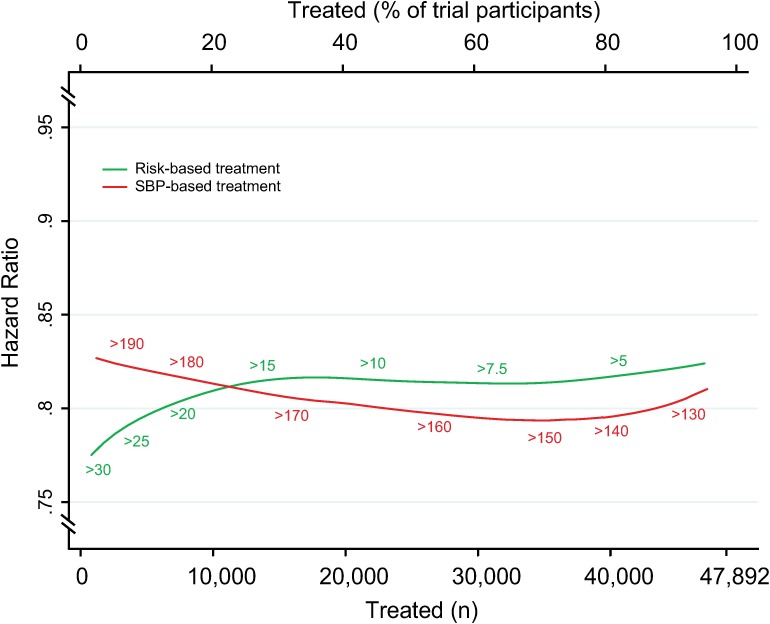
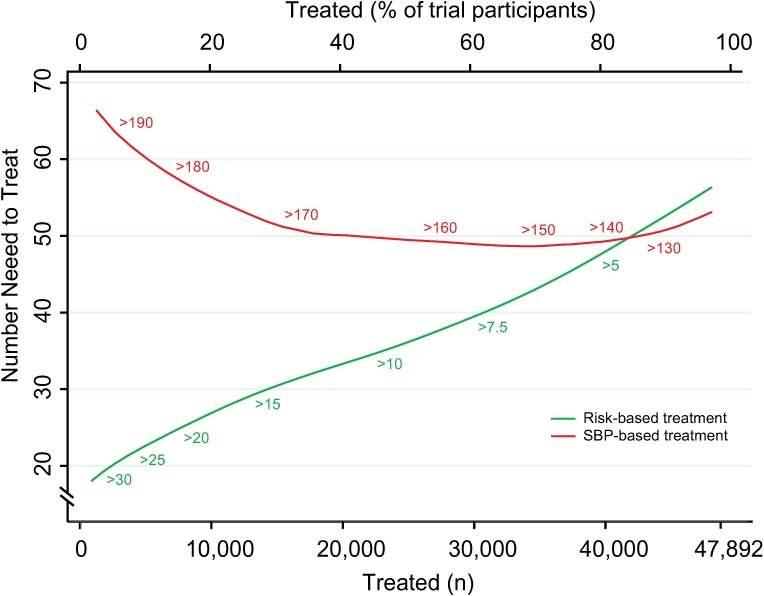
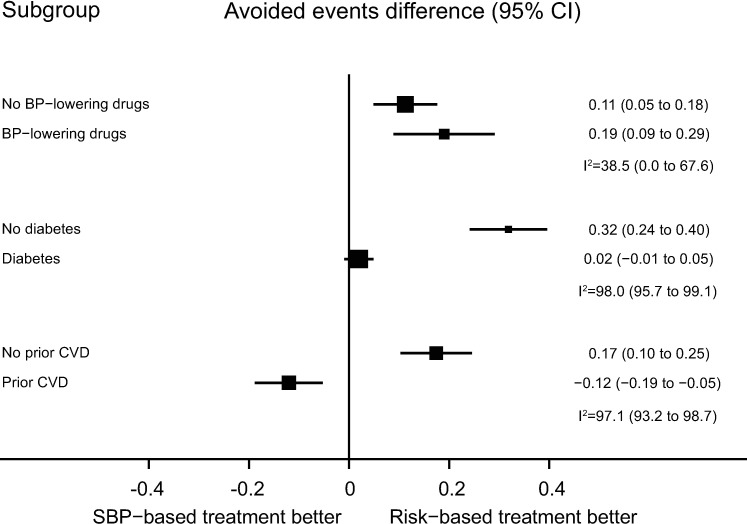
We used individual participant data from the Blood Pressure Lowering Treatment Trialists' Collaboration (BPLTTC) from 1995 to 2013. Trials randomly assigned participants to either blood pressure-lowering drugs versus placebo or more intensive versus less intensive blood pressure-lowering regimens. We estimated 5-y risk of CVD events using a multivariable Weibull model previously developed in this dataset. We compared the two strategies at specific SBP thresholds and across the spectrum of risk and blood pressure levels studied in BPLTTC trials. The primary outcome was number of CVD events avoided per persons treated. We included data from 11 trials (47,872 participants). During a median of 4.0 y of follow-up, 3,566 participants (7.5%) experienced a major cardiovascular event. Areas under the curve comparing the two treatment strategies throughout the range of possible thresholds for CVD risk and SBP demonstrated that, on average, a greater number of CVD events would be avoided for a given number of persons treated with the CVD risk strategy compared with the SBP strategy (area under the curve 0.71 [95% confidence interval (CI) 0.70-0.72] for the CVD risk strategy versus 0.54 [95% CI 0.53-0.55] for the SBP strategy). Compared with treating everyone with SBP ≥ 150 mmHg, a CVD risk strategy would require treatment of 29% (95% CI 26%-31%) fewer persons to prevent the same number of events or would prevent 16% (95% CI 14%-18%) more events for the same number of persons treated. Compared with treating everyone with SBP ≥ 140 mmHg, a CVD risk strategy would require treatment of 3.8% (95% CI 12.5% fewer to 7.2% more) fewer persons to prevent the same number of events or would prevent 3.1% (95% CI 1.5%-5.0%) more events for the same number of persons treated, although the former estimate was not statistically significant. In subgroup analyses, the CVD risk strategy did not appear to be more beneficial than the SBP strategy in patients with diabetes mellitus or established CVD.
A blood pressure-lowering treatment strategy based on predicted cardiovascular risk is more effective than one based on blood pressure levels alone across a range of thresholds. These results support using cardiovascular risk assessment to guide blood pressure treatment decision-making in moderate- to high-risk individuals, particularly for primary prevention.
临床实践指南传统上主要基于血压阈值来推荐降压治疗。相比之下,使用预测心血管风险已被提倡为一种更有效的策略,以指导心血管疾病(CVD)预防的治疗决策。我们旨在比较基于预测心血管风险的降压治疗策略与基于收缩压(SBP)水平的降压治疗策略的结果。
我们使用了来自 1995 年至 2013 年的降压治疗试验者协作组(BPLTTC)的个体参与者数据。试验随机将参与者分配到降压药物治疗组与安慰剂组,或更强化的降压治疗组与不太强化的降压治疗组。我们使用先前在该数据集开发的多变量 Weibull 模型来估计 5 年 CVD 事件风险。我们在特定 SBP 阈值和 BPLTTC 试验研究的风险和血压水平范围内比较了两种策略。主要结局是每治疗一人避免的 CVD 事件数。我们纳入了 11 项试验(47872 名参与者)的数据。在中位 4.0 年的随访期间,3566 名参与者(7.5%)发生了主要心血管事件。在可能的 CVD 风险和 SBP 阈值范围内比较两种治疗策略的曲线下面积表明,平均而言,与 SBP 策略相比,采用 CVD 风险策略治疗,给定数量的人可避免更多的 CVD 事件(CVD 风险策略的曲线下面积为 0.71 [95%置信区间(CI)0.70-0.72],SBP 策略为 0.54 [95% CI 0.53-0.55])。与治疗所有 SBP≥150mmHg 的患者相比,CVD 风险策略需要治疗的患者人数减少 29%(95% CI 26%-31%),以预防相同数量的事件,或者治疗相同数量的患者可预防 16%(95% CI 14%-18%)的更多事件。与治疗所有 SBP≥140mmHg 的患者相比,CVD 风险策略需要治疗的患者人数减少 3.8%(95% CI 12.5%更少至 7.2%更多),以预防相同数量的事件,或者治疗相同数量的患者可预防 3.1%(95% CI 1.5%-5.0%)的更多事件,尽管前者的估计值无统计学意义。在亚组分析中,在糖尿病或已确诊的 CVD 患者中,CVD 风险策略似乎不如 SBP 策略更有益。
基于预测心血管风险的降压治疗策略在一系列阈值范围内比基于血压水平的策略更有效。这些结果支持使用心血管风险评估来指导中高危个体的血压治疗决策,特别是在一级预防中。