Zhou Yu, Zhou Zhenyu, Liu Lifeng, Cao Xuecheng
Department of Orthopedics, General Hospital of Jinan Military Command, Jinan, 250031, China.
Present address: Department of Orthopedics, Civil Aviation Hospital of Shanghai, Shanghai, 200025, China.
J Med Case Rep. 2018 Mar 21;12(1):74. doi: 10.1186/s13256-018-1609-z.
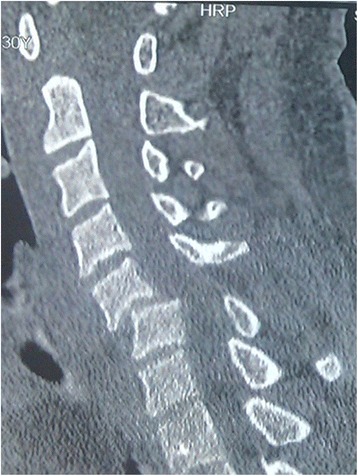
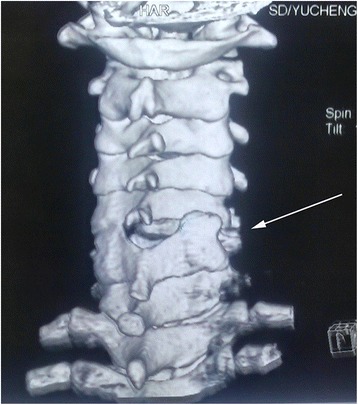
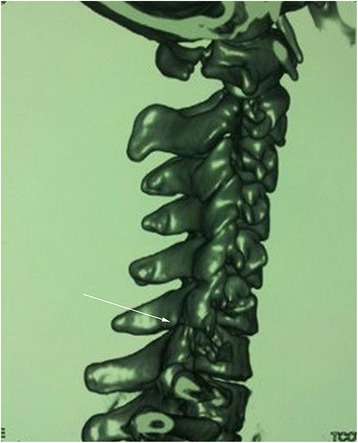
Skeletal and soft tissue damage are often associated with unilateral facet dislocations, which undoubtedly lead to instability of the spine and further increase difficulties in cervical reduction. This type of irreducible facet dislocation is usually accompanied with potential catastrophic consequences including neurological deficit and severe disability. Therefore, a consistent and evidence-based treatment plan is imperative.
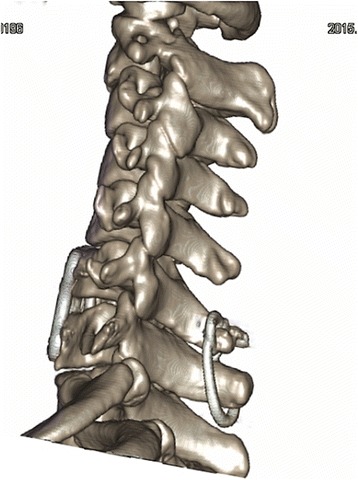
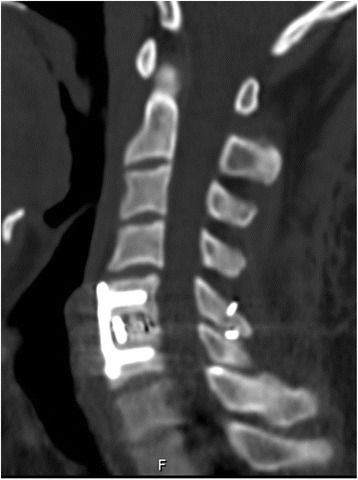
The literature regarding the management of traumatic unilateral locked cervical facet dislocations was reviewed. Two patient cases (a 30-year-old Asian man and a 25-year-old Asian woman) who suffered irreducible cervical facet dislocations were presented. These two patients received surgical treatments including posterior reduction by poking facet joints, adjacent spinous process fixation by wire rope banding, anterior plate fixation, and intervertebral fusion after the failure of skull traction and closed reduction. At the postoperative 24-month follow-up, intervertebral fusion was achieved and our patients' neurological status improved based on the American Spinal Injury Association scale, compared with their preoperative status.
Unilateral facet joint dislocations of subaxial cervical spine are difficult to reduce when complicated with posterior facet fractures or ligamentous injury. Magnetic resonance imaging can be beneficial for identifying ventral and dorsal compressive lesions, as well as ligamentous or capsule rupture. The combination of posterior reduction and anterior fixation with fusion has advantages in terms of clinical safety, ease of operation, and less iatrogenic damage.
骨骼和软组织损伤常与单侧小关节脱位相关,这无疑会导致脊柱不稳定,并进一步增加颈椎复位的难度。这种不可复位的小关节脱位通常伴有潜在的灾难性后果,包括神经功能缺损和严重残疾。因此,制定一个一致且基于证据的治疗方案势在必行。
回顾了有关创伤性单侧锁定颈椎小关节脱位治疗的文献。介绍了两例不可复位颈椎小关节脱位患者的病例(一名30岁亚洲男性和一名25岁亚洲女性)。这两名患者在颅骨牵引和闭合复位失败后接受了手术治疗,包括通过戳拨小关节进行后路复位、用钢丝绳捆绑相邻棘突进行固定、前路钢板固定和椎间融合。术后24个月随访时,实现了椎间融合,与术前状态相比,根据美国脊髓损伤协会量表,患者的神经状态有所改善。
下颈椎单侧小关节脱位合并后关节面骨折或韧带损伤时难以复位。磁共振成像有助于识别腹侧和背侧压迫性病变以及韧带或关节囊破裂。后路复位与前路固定融合相结合在临床安全性、操作简便性和医源性损伤较小方面具有优势。