Breitve Monica H, Chwiszczuk Luiza J, Brønnick Kolbjørn, Hynninen Minna J, Auestad Bjørn H, Aarsland Dag, Rongve Arvid
Department of Research and Innovation, Helse-Fonna Haugesund Hospital, Haugesund, Norway.
Department of Geriatric Psychiatry, Clinic of Psychiatry, Helse-Fonna Haugesund Hospital, Haugesund, Norway.
Front Neurol. 2018 Mar 6;9:124. doi: 10.3389/fneur.2018.00124. eCollection 2018.
There are relatively few longitudinal studies on the differences in cognitive decline between Alzheimer's disease (AD) and dementia with Lewy bodies (DLB), and the majority of existing studies have suboptimal designs.
We investigated the differences in cognitive decline in AD compared to DLB over 4 years and cognitive domain predictors of progression.
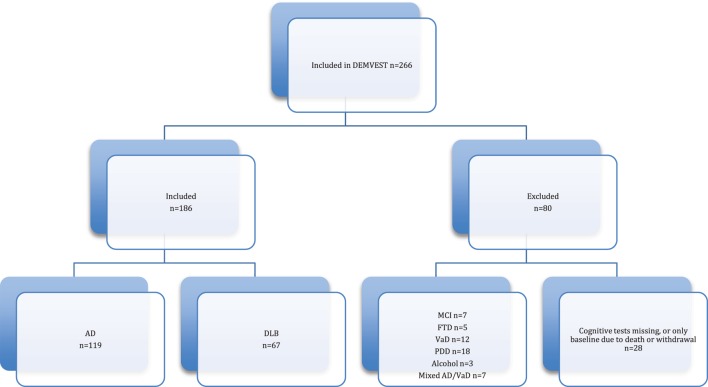
In a longitudinal study, 266 patients with first-time diagnosis of mild dementia were included and followed annually. The patients were tested annually with neuropsychological tests and screening instruments [MMSE (Mini-Mental Status Examination), Clinical Dementia Rating (CDR), the second edition of California Verbal Learning Test (CVLT-II), Trail Making Test A & B (TMT A & B), Stroop test, Controlled Oral Word Associations Test (COWAT) animal naming, Boston Naming Test, Visual Object and Space Perception Battery (VOSP) Cubes and Silhouettes]. Longitudinal analyses were performed with linear mixed effects (LME) models and Cox regression. Both specific neuropsychological tests and cognitive domains were analyzed.
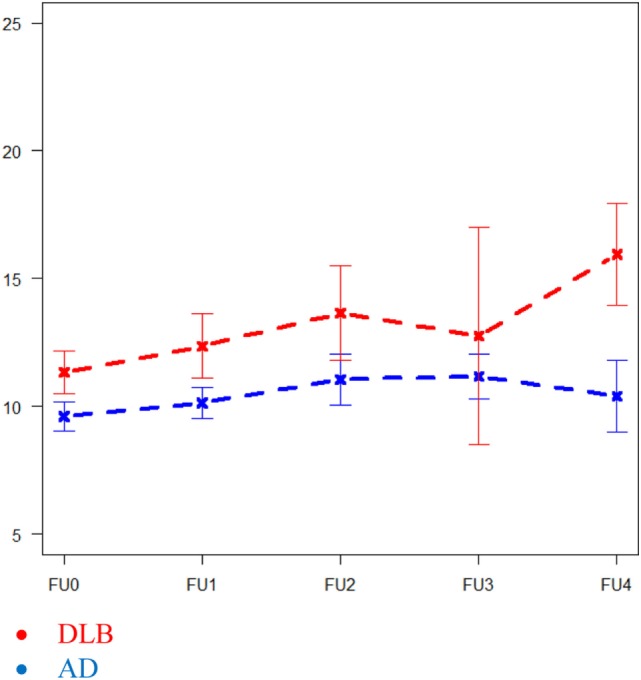
This study sample comprised 119 AD and 67 DLB patients. In TMT A, the DLB patients had a faster decline over 4 years than patients with AD ( = 0.013). No other longitudinal differences in specific neuropsychological tests were found. Higher executive domain scores at baseline were associated with a longer time to reach severe dementia (CDR = 3) or death for the total sample ( = 0.032). High or low visuospatial function at baseline was not found to be associated with cognitive decline (MMSE) or progression of dementia severity (CDR) over time.
Over 4 years, patients with DLB had a faster decline in TMT A than patients with AD, but this should be interpreted cautiously. Beyond this, there was little support for faster decline in DLB patients neuropsychologically than in AD patients.
关于阿尔茨海默病(AD)和路易体痴呆(DLB)认知衰退差异的纵向研究相对较少,且大多数现有研究设计欠佳。
我们研究了AD与DLB在4年期间认知衰退的差异以及病情进展的认知领域预测因素。
在一项纵向研究中,纳入了266例首次诊断为轻度痴呆的患者,并每年进行随访。每年使用神经心理学测试和筛查工具[简易精神状态检查表(MMSE)、临床痴呆评定量表(CDR)、加利福尼亚语言学习测验第二版(CVLT-II)、连线测验A和B(TMT A和B)、斯特鲁普测验、受控口语词语联想测验(COWAT)动物命名、波士顿命名测验、视觉物体与空间感知成套测验(VOSP)立方体和轮廓图]对患者进行测试。采用线性混合效应(LME)模型和Cox回归进行纵向分析。对特定神经心理学测试和认知领域均进行了分析。
本研究样本包括119例AD患者和67例DLB患者。在TMT A中,DLB患者在4年期间的衰退速度比AD患者更快(=0.013)。在特定神经心理学测试中未发现其他纵向差异。对于整个样本,基线时较高的执行领域得分与达到重度痴呆(CDR = 3)或死亡的时间较长相关(=0.032)。未发现基线时高或低的视觉空间功能与认知衰退(MMSE)或痴呆严重程度进展(CDR)随时间的变化相关。
在4年期间,DLB患者在TMT A中的衰退速度比AD患者更快,但对此应谨慎解读。除此之外,几乎没有证据支持DLB患者在神经心理学方面的衰退速度比AD患者更快。