Dossou Jean-Paul, Cresswell Jenny A, Makoutodé Patrick, De Brouwere Vincent, Witter Sophie, Filippi Veronique, Kanhonou Lydie G, Goufodji Sourou B, Lange Isabelle L, Lawin Lionel, Affo Fabien, Marchal Bruno
Department of Public Health, Research Centre in Human Reproduction and Demography, Cotonou, Benin.
Department of Public Health, Institute of Tropical Medicine, Antwerp, Belgium.
BMJ Glob Health. 2018 Jan 29;3(1):e000537. doi: 10.1136/bmjgh-2017-000537. eCollection 2018.
In 2009, the Benin government introduced a user fee exemption policy for caesarean sections. We analyse this policy with regard to how the existing ideas and institutions related to user fees influenced key steps of the policy cycle and draw lessons that could inform the policy dialogue for universal health coverage in the West African region.
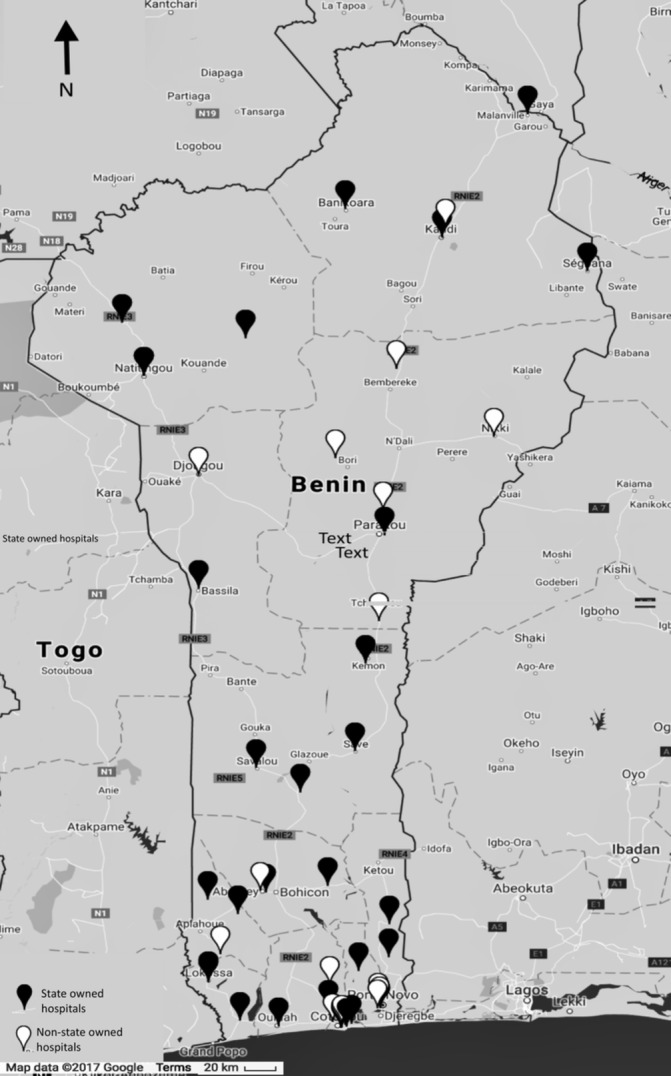
Following the policy stages model, we analyse the agenda setting, policy formulation and legitimation phase, and assess the implementation fidelity and policy results. We adopted an embedded case study design, using quantitative and qualitative data collected with 13 tools at the national level and in seven hospitals implementing the policy.
We found that the initial political goal of the policy was not to reduce maternal mortality but to eliminate the detention in hospitals of mothers and newborns who cannot pay the user fees by exempting a comprehensive package of maternal health services. We found that the policy development process suffered from inadequate uptake of evidence and that the policy content and process were not completely in harmony with political and public health goals. The initial policy intention clashed with the neoliberal orientation of the political system, the fee recovery principles institutionalised since the Bamako Initiative and the prevailing ideas in favour of user fees. The policymakers did not take these entrenched factors into account. The resulting tension contributed to a benefit package covering only caesarean sections and to the variable implementation and effectiveness of the policy.
The influence of organisational culture in the decision-making processes in the health sector is often ignored but must be considered in the design and implementation of any policy aimed at achieving universal health coverage in West African countries.
2009年,贝宁政府出台了剖宫产手术费用减免政策。我们分析这项政策,关注与费用相关的现有观念和制度如何影响政策周期的关键步骤,并汲取经验教训,为西非地区全民健康覆盖的政策对话提供参考。
遵循政策阶段模型,我们分析议程设定、政策制定与合法化阶段,并评估实施的保真度和政策结果。我们采用嵌入式案例研究设计,运用通过13种工具在国家层面以及7家实施该政策的医院收集的定量和定性数据。
我们发现,该政策最初的政治目标并非降低孕产妇死亡率,而是通过免除一揽子孕产妇保健服务费用,消除医院对无力支付费用的母亲和新生儿的滞留现象。我们发现,政策制定过程存在证据采纳不足的问题,政策内容和过程与政治及公共卫生目标并不完全契合。最初的政策意图与政治体制的新自由主义倾向、自《巴马科倡议》以来制度化的费用回收原则以及支持收取费用的主流观念发生冲突。政策制定者没有考虑到这些根深蒂固的因素。由此产生的紧张关系导致福利包仅涵盖剖宫产手术,以及政策实施的差异和效果不佳。
卫生部门决策过程中组织文化的影响常常被忽视,但在旨在实现西非国家全民健康覆盖的任何政策的设计和实施中都必须予以考虑。