Department of Clinical Sciences, Danderyd Hospital, Karolinska Institutet, Building 8-9, 6th floor, 18288, Stockholm, Sweden.
Department of Molecular Medicine and Surgery, Karolinska Institutet, Stockholm, Sweden.
J Thromb Thrombolysis. 2018 May;45(4):477-485. doi: 10.1007/s11239-018-1642-1.
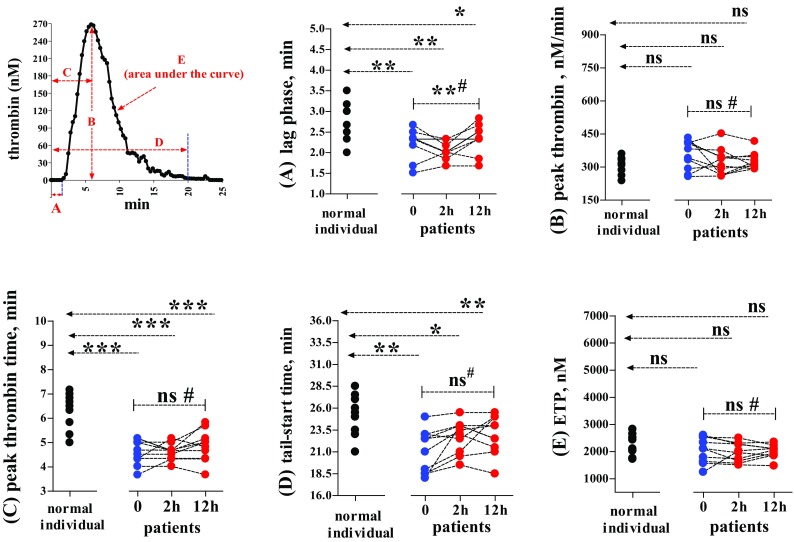
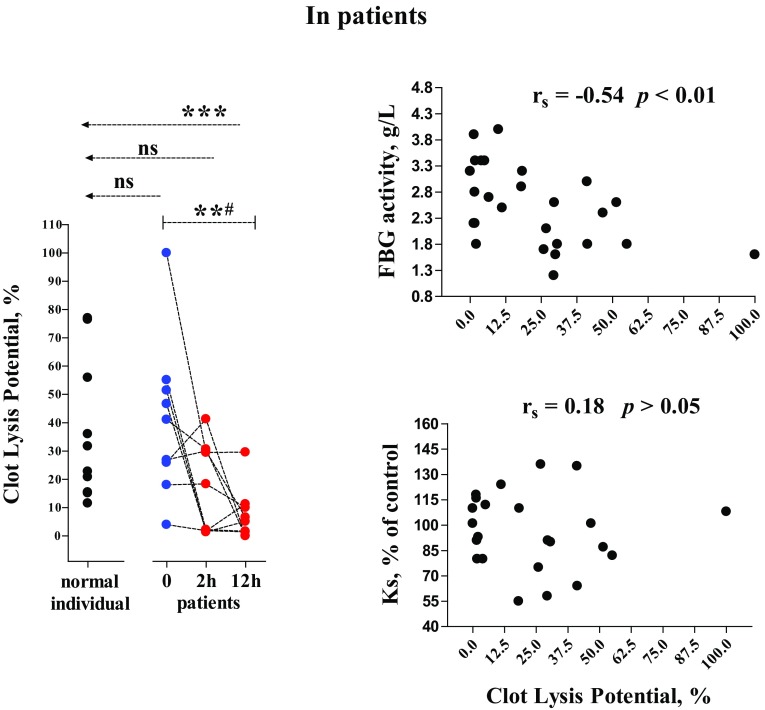
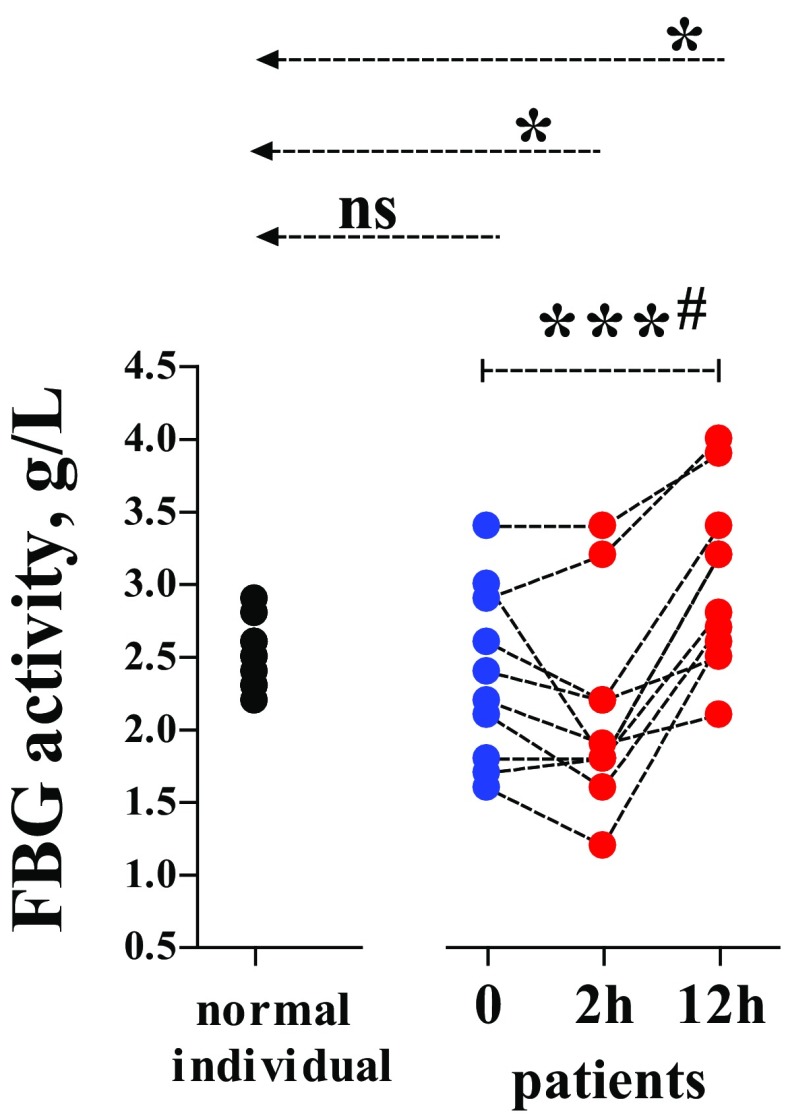
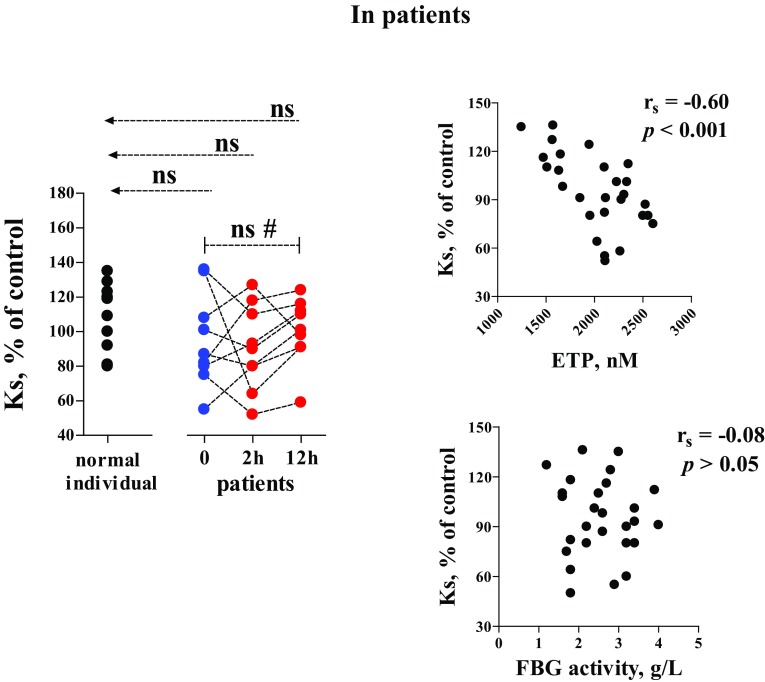
Acute traumatic coagulopathy (ATC) diagnosed by prolongation of APTT and/or PT/INR involves alterations in platelet activity, coagulation and fibrinolysis. However, data showing the haemostatic situation in injured patients without ATC are scarce. To assess whether haemostatic impairment is also present in injured patients without ATC, ten injured patients without ATC and ten normal individuals were examined. The patients were sampled on arrival at the emergency department 0, 2, 12 h after surgical or other intervention. Thrombin generation, fibrin formation and fibrin proteolysis were determined via several laboratory methods, using tissue factor as the coagulation trigger. Thrombograms demonstrated that trauma accelerated both thrombin generation and decay. In the presence of unaffected peak thrombin levels, these two contradictory effects cancelled each other out, leading to the global endogenous thrombin potential (ETP) remaining normal. Under the mediation of normal ETP, fibrin network permeability (Ks) kept the reference levels in the two groups of subjects. Fibrinogen (FBG) activity (Clauss) rose with time from 0 to 2 h and 12 h, which significantly slowed down Clot Lysis Potential as determined by an in vitro method with exogenous t-PA.
the main haemostatic impairment in the present patients concerned an increased tendency in FBG activity. Since an increase in FBG is a biomarker of acute inflammation and also predicts greater fibrin production which down-regulates fibrinolysis, we suggest that during early stages after injury, patients without ATC may suffer from worsening inflammation and confront enhancement of thrombosis risk due to dysfunction of fibrinolysis.
通过延长 APTT 和/或 PT/INR 诊断的急性创伤性凝血病(ATC)涉及血小板活性、凝血和纤维蛋白溶解的改变。然而,目前尚无关于无 ATC 创伤患者止血情况的数据。为了评估无 ATC 的创伤患者是否也存在止血障碍,我们检查了 10 名无 ATC 的创伤患者和 10 名正常个体。患者在到达急诊室时(0 小时)、手术或其他干预后 2 小时和 12 小时进行采样。通过几种实验室方法,使用组织因子作为凝血触发物,测定凝血酶生成、纤维蛋白形成和纤维蛋白水解。血栓图显示创伤加速了凝血酶的生成和衰减。在不受影响的峰值凝血酶水平存在的情况下,这两种矛盾的作用相互抵消,导致全球内源性凝血酶潜力(ETP)保持正常。在正常 ETP 的介导下,纤维蛋白网络通透性(Ks)使两组受试者的参考水平保持正常。纤维蛋白原(FBG)活性(Clauss)从 0 小时到 2 小时和 12 小时逐渐升高,这显著减缓了通过体外方法用外源性 t-PA 测定的凝块溶解潜能。
目前患者的主要止血障碍是 FBG 活性增加。由于 FBG 的增加是急性炎症的生物标志物,也预测了更多的纤维蛋白生成,这会下调纤维蛋白溶解,因此我们建议,在受伤后的早期阶段,无 ATC 的患者可能会因炎症加重而遭受更多的痛苦,并因纤维蛋白溶解功能障碍而面临血栓形成风险的增加。