White N J, Contaifer D, Martin E J, Newton J C, Mohammed B M, Bostic J L, Brophy G M, Spiess B D, Pusateri A E, Ward K R, Brophy D F
Department of Medicine/Division of Emergency Medicine, University of Washington, and Puget Sound Blood Center Research Institute, Seattle, WA, USA.
Coagulation Advancement Laboratory, Department of Pharmacotherapy and Outcomes Science, Virginia Commonwealth University, Richmond, VA, USA.
J Thromb Haemost. 2015 Jun;13(6):978-88. doi: 10.1111/jth.12919. Epub 2015 May 9.
Trauma-induced coagulopathy is a complex multifactorial hemostatic response that is poorly understood.
To identify distinct hemostatic responses to trauma and identify key components of the hemostatic system that vary between responses.
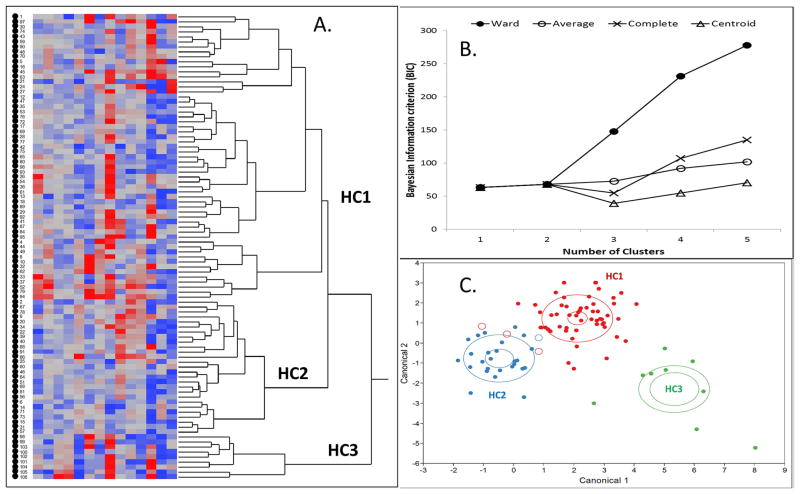
PATIENTS/METHODS: A cross-sectional observational study of adult trauma patients at an urban level I trauma center emergency department was performed. Hierarchical clustering analysis was used to identify distinct clusters of similar subjects according to vital signs, injury/shock severity, and comprehensive assessment of coagulation, clot formation, platelet function, and thrombin generation.
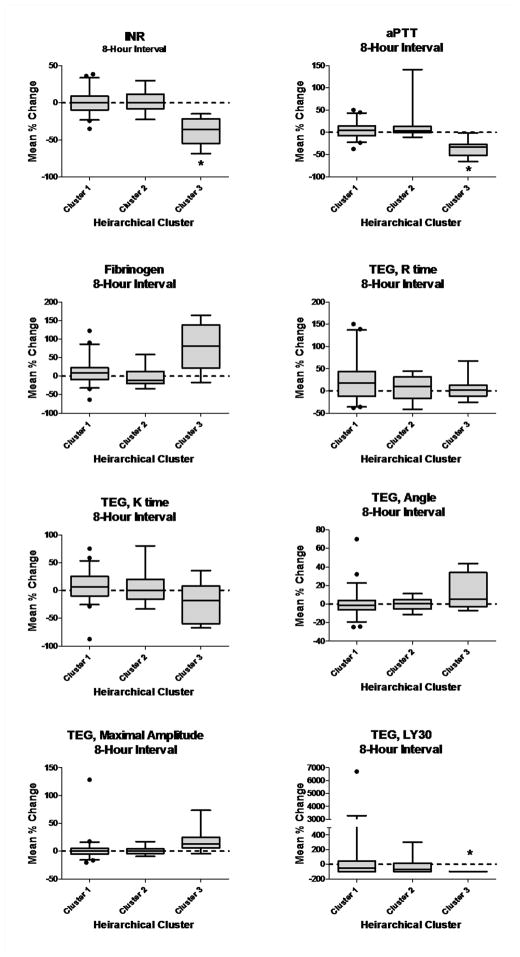
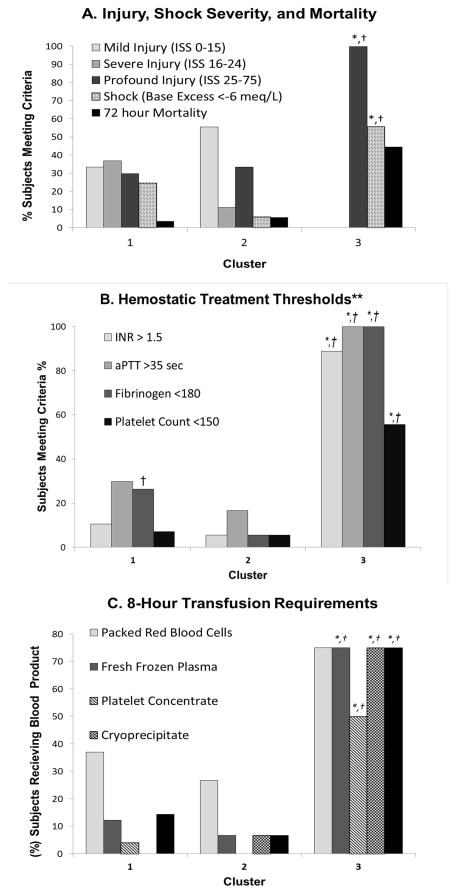
Among 84 total trauma patients included in the model, three distinct trauma clusters were identified. Cluster 1 (N = 57) showed platelet activation, preserved peak thrombin generation, plasma coagulation dysfunction, a moderately decreased fibrinogen concentration and normal clot formation relative to healthy controls. Cluster 2 (N = 18) showed platelet activation, preserved peak thrombin generation, and a preserved fibrinogen concentration with normal clot formation. Cluster 3 (N = 9) was the most severely injured and shocked, and showed a strong inflammatory and bleeding phenotype. Platelet dysfunction, thrombin inhibition, plasma coagulation dysfunction and a decreased fibrinogen concentration were present in this cluster. Fibrinolytic activation was present in all clusters, but was particularly increased in cluster 3. Trauma clusters were most noticeably different in their relative fibrinogen concentration, peak thrombin generation, and platelet-induced clot contraction.
Hierarchical clustering analysis identified three distinct hemostatic responses to trauma. Further insights into the underlying hemostatic mechanisms responsible for these responses are needed.
创伤性凝血病是一种复杂的多因素止血反应,目前对其了解甚少。
确定对创伤的不同止血反应,并识别在不同反应之间变化的止血系统关键成分。
患者/方法:在一家城市一级创伤中心急诊科对成年创伤患者进行了横断面观察研究。采用层次聚类分析,根据生命体征、损伤/休克严重程度以及对凝血、血栓形成、血小板功能和凝血酶生成的综合评估,识别相似受试者的不同聚类。
在纳入模型的84例创伤患者中,识别出三个不同的创伤聚类。聚类1(N = 57)表现为血小板激活、凝血酶生成峰值保留、血浆凝血功能障碍、纤维蛋白原浓度中度降低以及相对于健康对照的正常血栓形成。聚类2(N = 18)表现为血小板激活、凝血酶生成峰值保留以及纤维蛋白原浓度保留和正常血栓形成。聚类3(N = 9)是受伤和休克最严重的,表现出强烈的炎症和出血表型。该聚类存在血小板功能障碍、凝血酶抑制、血浆凝血功能障碍和纤维蛋白原浓度降低。所有聚类中均存在纤溶激活,但在聚类3中尤其增加。创伤聚类在相对纤维蛋白原浓度、凝血酶生成峰值和血小板诱导的血块收缩方面差异最为明显。
层次聚类分析确定了对创伤的三种不同止血反应。需要进一步深入了解导致这些反应的潜在止血机制。