Center for Observational Research (CfOR), 1 Amgen Center Drive, MS 24-2-A, Thousand Oaks, CA, 91320, USA.
Department of Medicine, University of California, San Francisco, CA, USA.
Arch Osteoporos. 2018 Mar 21;13(1):33. doi: 10.1007/s11657-018-0439-3.
Studies examining real-world effectiveness of osteoporosis therapies are beset by limitations due to confounding by indication. By evaluating longitudinal changes in fracture incidence, we demonstrated that osteoporosis therapies are effective in reducing fracture risk in real-world practice settings.
Osteoporosis therapies have been shown to reduce incidence of vertebral and non-vertebral fractures in placebo-controlled randomized clinical trials. However, information on the real-world effectiveness of these therapies is limited.
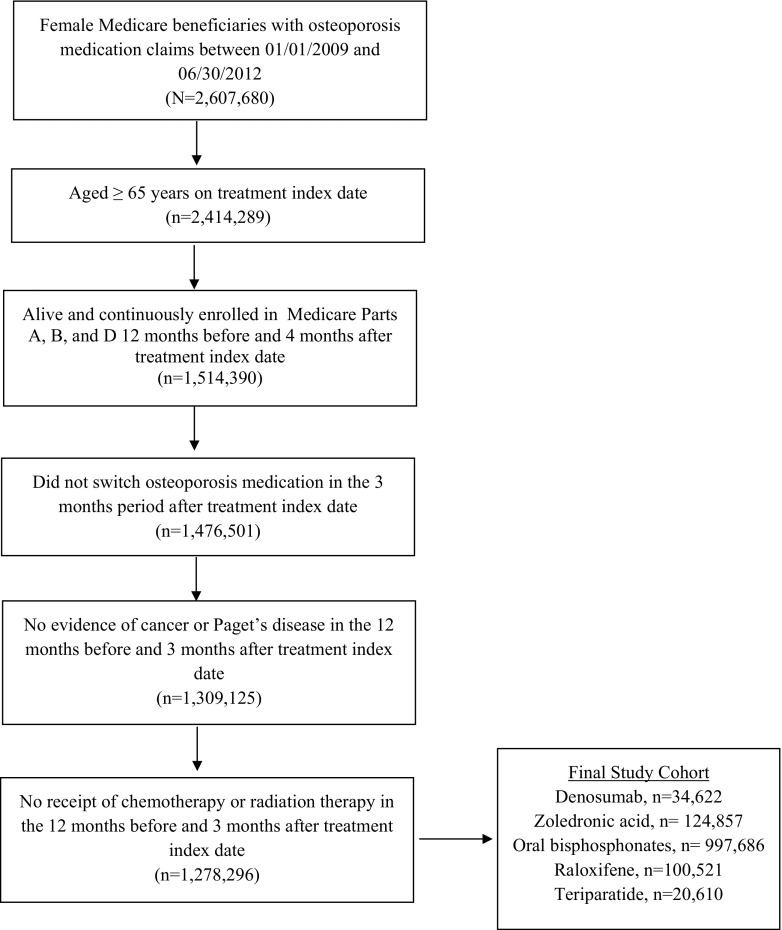
We examined fracture risk reduction in older, post-menopausal women treated with osteoporosis therapies. Using Medicare claims, we identified 1,278,296 women age ≥ 65 years treated with zoledronic acid, oral bisphosphonates, denosumab, teriparatide, or raloxifene. Fracture incidence rates before and after treatment initiation were described to understand patients' fracture risk profile, and fracture reduction effectiveness of each therapy was evaluated as a longitudinal change in incidence rates.
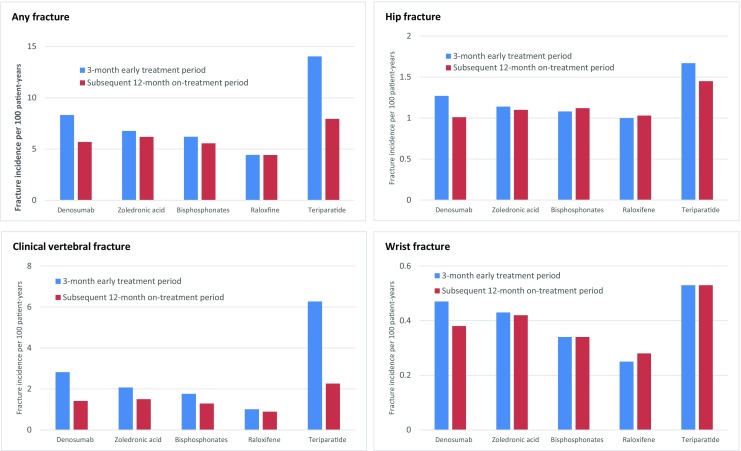
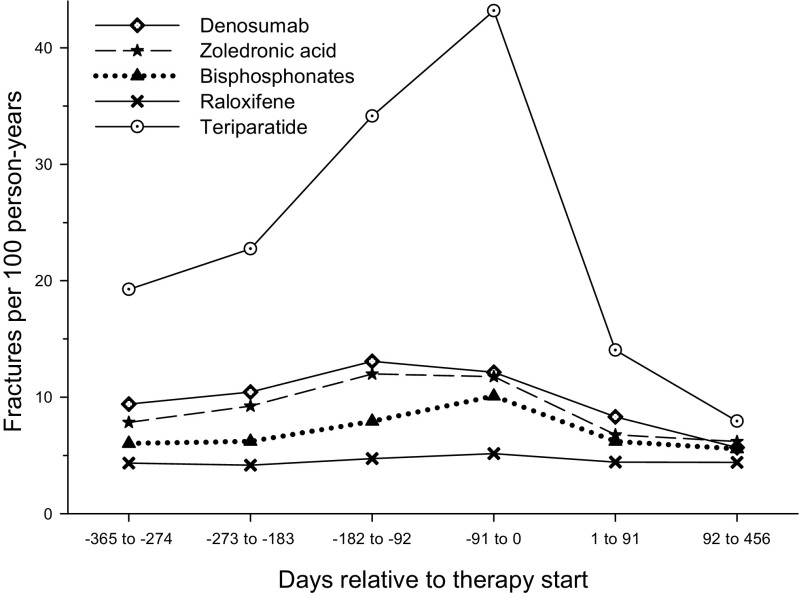
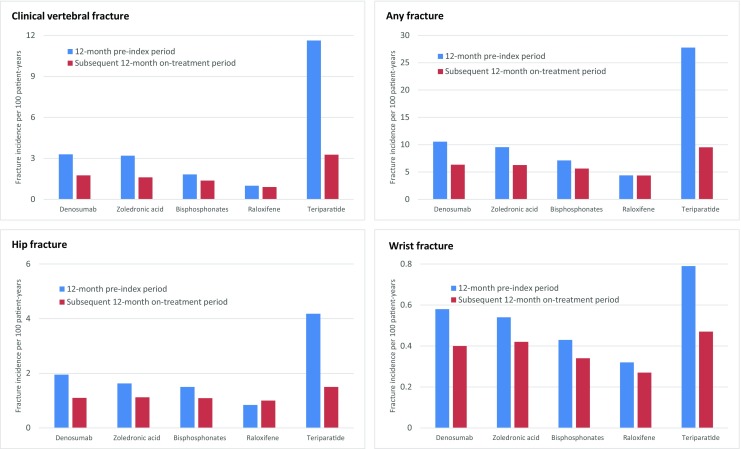
Fracture incidence rates increased during the period leading up to treatment initiation and were highest in the 3-month period most proximal to treatment initiation. Fracture incidence rates following treatment initiation were significantly lower than before treatment initiation. Compared with the 12-month pre-index period, there were reductions in clinical vertebral fractures for denosumab (45%; 95% confidence interval [CI] 39-51%), zoledronic acid (50%; 95% CI 47-52%), oral bisphosphonates (24%; 95% CI 22-26%), and teriparatide (72%; 95% CI 69-75%) during the subsequent 12 months. Relative to the first 3 months after initiation, clinical vertebral fractures were reduced for denosumab (51%; 95% CI 42-59%), zoledronic acid (25%; 95% CI 17-32%), oral bisphosphonates (23%; 95% CI 20-26%), and teriparatide (64%; 95% CI 58-69%) during the subsequent 12 months.
In summary, reductions in fracture incidence over time were observed in cohorts of patients treated with osteoporosis therapies.
由于混杂因素的影响,研究骨质疏松症治疗的真实世界疗效受到了限制。通过评估骨折发生率的纵向变化,我们证明了骨质疏松症治疗在真实世界的实践环境中可以有效地降低骨折风险。
在安慰剂对照的随机临床试验中,骨质疏松症治疗已被证明可以降低椎体和非椎体骨折的发生率。然而,关于这些治疗方法在真实世界中的有效性的信息是有限的。
我们研究了接受骨质疏松症治疗的老年绝经后妇女的骨折风险降低情况。我们使用医疗保险索赔数据,确定了 1278296 名年龄≥65 岁的接受唑来膦酸、口服双膦酸盐、地舒单抗、特立帕肽或雷洛昔芬治疗的女性。描述了治疗前和治疗开始后骨折发生率的变化,以了解患者的骨折风险特征,并评估每种治疗方法的骨折减少效果,作为发生率的纵向变化。
在治疗开始前的一段时间内,骨折发生率增加,在最接近治疗开始的 3 个月内达到最高。治疗开始后,骨折发生率明显低于治疗前。与 12 个月的索引前时期相比,地舒单抗(45%;95%置信区间[CI] 39-51%)、唑来膦酸(50%;95%CI 47-52%)、口服双膦酸盐(24%;95%CI 22-26%)和特立帕肽(72%;95%CI 69-75%)的临床椎体骨折发生率在随后的 12 个月中降低。与治疗开始后前 3 个月相比,地舒单抗(51%;95%CI 42-59%)、唑来膦酸(25%;95%CI 17-32%)、口服双膦酸盐(23%;95%CI 20-26%)和特立帕肽(64%;95%CI 58-69%)的临床椎体骨折发生率在随后的 12 个月中降低。
总之,在接受骨质疏松症治疗的患者队列中,随着时间的推移,骨折发生率有所下降。