Cameron David, Ubels Jasper, Norström Fredrik
a Department of Public Health and Clinical Medicine , Umeå University , Umeå , Sweden.
Glob Health Action. 2018;11(1):1447828. doi: 10.1080/16549716.2018.1447828.
The amount a government should be willing to invest in adopting new medical treatments has long been under debate. With many countries using formal cost-effectiveness (C/E) thresholds when examining potential new treatments and ever-growing medical costs, accurately setting the level of a C/E threshold can be essential for an efficient healthcare system.
The aim of this systematic review is to describe the prominent approaches to setting a C/E threshold, compile available national-level C/E threshold data and willingness-to-pay (WTP) data, and to discern whether associations exist between these values, gross domestic product (GDP) and health-adjusted life expectancy (HALE). This review further examines current obstacles faced with the presently available data.
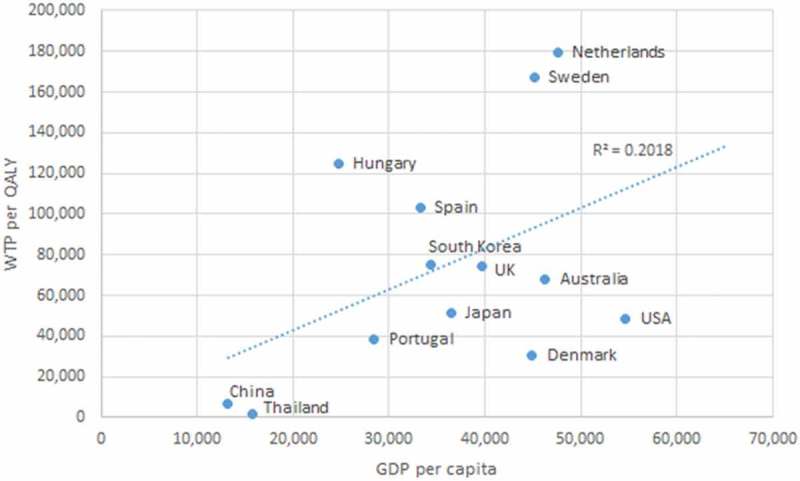
A systematic review was performed to collect articles which have studied national C/E thresholds and willingness-to-pay (WTP) per quality-adjusted life year (QALY) in the general population. Associations between GDP, HALE, WTP, and C/E thresholds were analyzed with correlations.
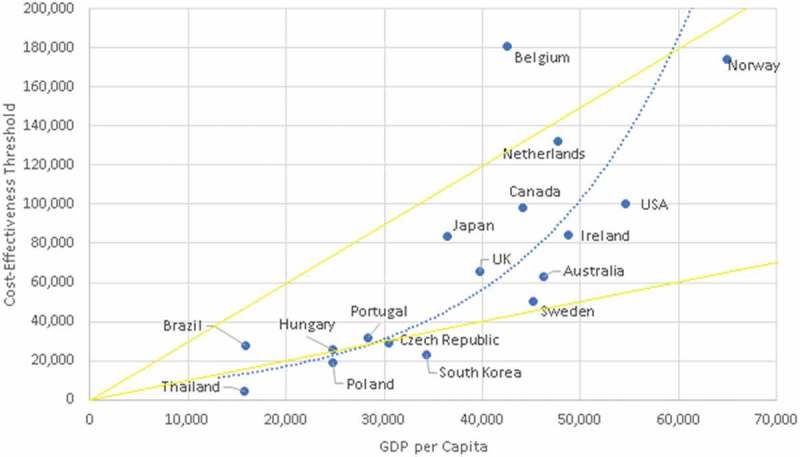
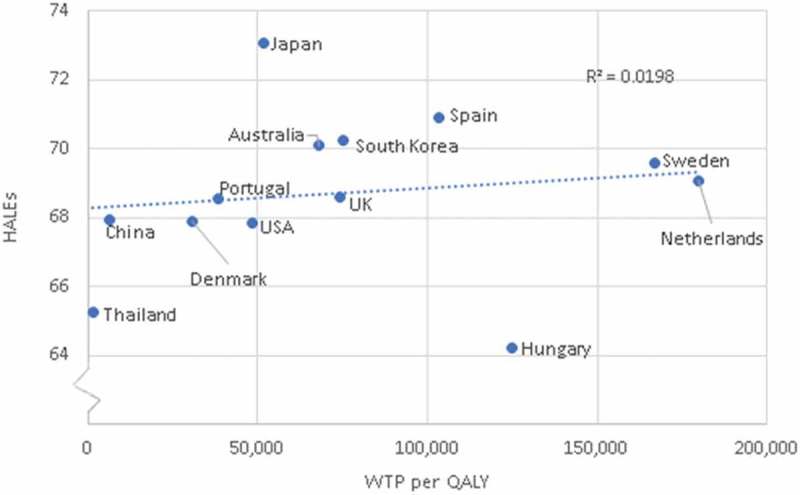
Seventeen countries were identified from nine unique sources to have formal C/E thresholds within our inclusion criteria. Thirteen countries from nine sources were identified to have WTP per QALY data within our inclusion criteria. Two possible associations were identified: C/E thresholds with HALE (quadratic correlation of 0.63), and C/E thresholds with GDP per capita (polynomial correlation of 0.84). However, these results are based on few observations and therefore firm conclusions cannot be made.
Most national C/E thresholds identified in our review fall within the WHO's recommended range of one-to-three times GDP per capita. However, the quality and quantity of data available regarding national average WTP per QALY, opportunity costs, and C/E thresholds is poor in comparison to the importance of adequate investment in healthcare. There exists an obvious risk that countries might either over- or underinvest in healthcare if they base their decision-making process on erroneous presumptions or non-evidence-based methodologies. The commonly referred to value of 100,000$ USD per QALY may potentially have some basis.
政府愿意投资采用新医疗疗法的金额长期以来一直存在争议。许多国家在审查潜在的新疗法时使用正式的成本效益(C/E)阈值,且医疗成本不断攀升,准确设定C/E阈值水平对于高效的医疗保健系统至关重要。
本系统评价的目的是描述设定C/E阈值的主要方法,汇总可用的国家层面C/E阈值数据和支付意愿(WTP)数据,并辨别这些值、国内生产总值(GDP)和健康调整生命年(HALE)之间是否存在关联。本评价还进一步考察了现有数据面临的当前障碍。
进行了一项系统评价,以收集研究一般人群中全国C/E阈值和每质量调整生命年(QALY)支付意愿(WTP)的文章。通过相关性分析GDP、HALE、WTP和C/E阈值之间的关联。
从九个独特来源中确定有17个国家在我们的纳入标准内有正式的C/E阈值。从九个来源中确定有13个国家在我们的纳入标准内有每QALY的WTP数据。确定了两个可能的关联:C/E阈值与HALE(二次相关性为0.63),以及C/E阈值与人均GDP(多项式相关性为0.84)。然而,这些结果基于的观察数据较少,因此无法得出确凿结论。
我们的评价中确定的大多数国家C/E阈值落在世界卫生组织建议的人均GDP的一至三倍范围内。然而,与医疗保健充足投资的重要性相比,关于全国每QALY平均WTP、机会成本和C/E阈值的现有数据的质量和数量较差。如果各国基于错误的假设或非循证方法进行决策过程,存在明显的风险,即它们可能在医疗保健方面投资过多或过少。通常提到的每QALY 100,000美元的价值可能有一定依据。