Brosnahan Godela M, Abebe Kaleab Z, Moore Charity G, Bae Kyongtae T, Braun William E, Chapman Arlene B, Flessner Michael F, Harris Peter C, Hogan Marie C, Perrone Ronald D, Rahbari-Oskoui Frederic F, Steinman Theodore I, Torres Vicente E
University of Colorado Denver, Aurora, Colorado, CO, United States.
University of Pittsburgh, Pittsburgh, Pennsylvania, PA, United States.
Curr Hypertens Rev. 2018;14(1):39-47. doi: 10.2174/1573402114666180322110209.
The HALT PKD trial in early autosomal dominant polycystic kidney disease (ADPKD) showed that intensive control of systolic blood pressure to 95-110 mmHg was associated with a 14% slower rate of kidney volume growth compared to standard control. It is unclear whether this result was due to greater blockade of the renin-angiotensin-aldosterone system (RAAS) by allowing the use of higher drug doses in the low blood pressure arm, or due to the lower blood pressure per se.
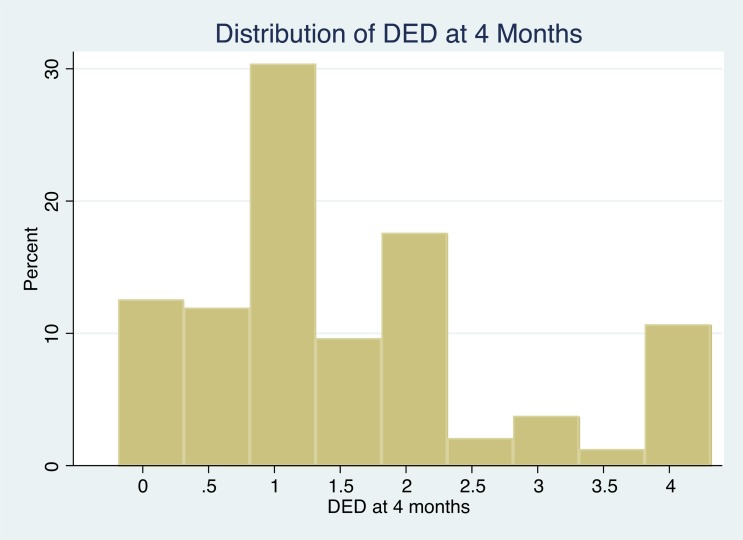
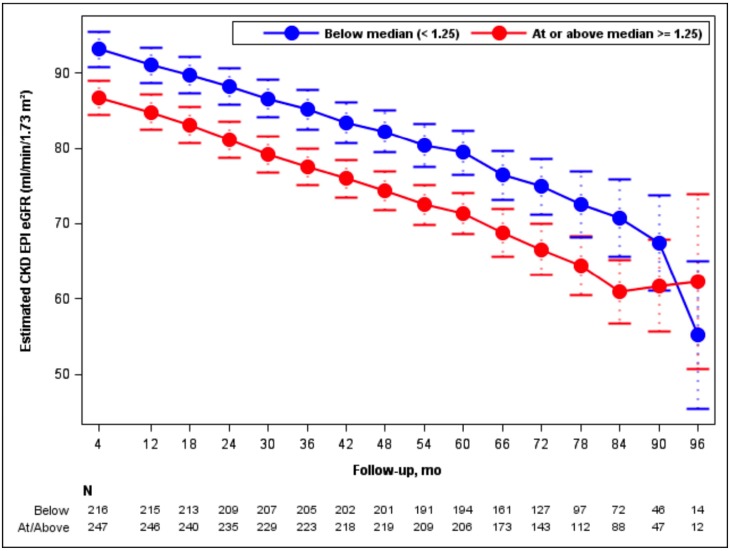
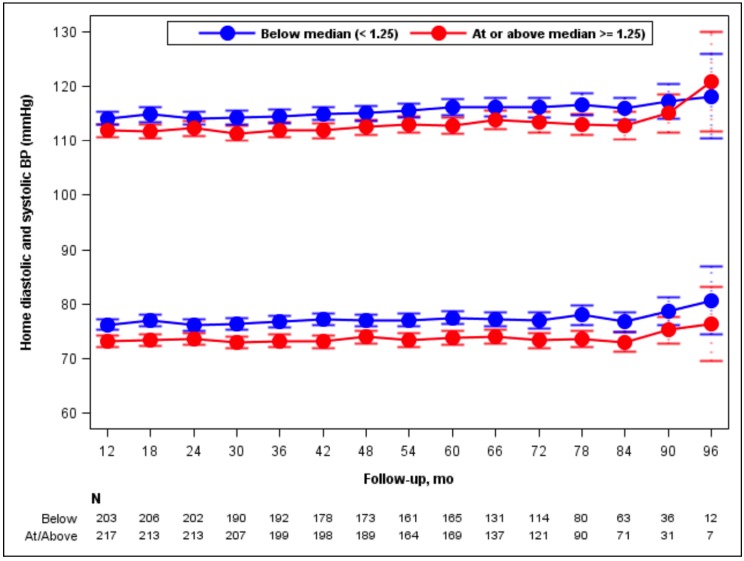
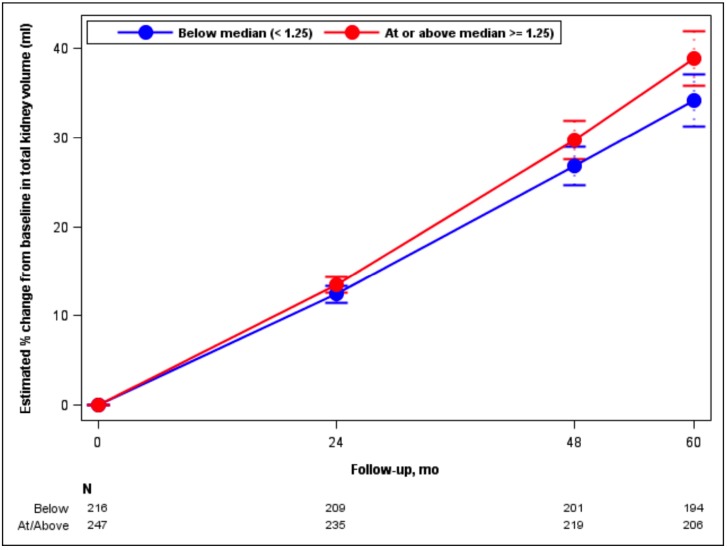
In this secondary analysis of HALT PKD Study A, we categorized participants into high and low dose groups based on the median daily equivalent dose of RAAS blocking drugs used after the initial dose titration period. Using linear mixed models, we compared the percent change in total kidney volume and the slope of estimated glomerular filtration rate (eGFR) between the 2 groups. We also assessed the effects of time-varying dose and time-varying blood pressure parameters on these outcomes.
Subjects in the high dose group (n=252) did not experience a slower increase in total kidney volume than those in the low-dose (n=225) group, after adjustment for age, sex, genotype, and BP arm. The chronic slope of eGFR decline was similar in the 2 groups. Higher time-varying systolic blood pressure was associated with a steeper decline in eGFR.
ADPKD progression (as detected by eGFR decline and TKV increase) was ameliorated by intense blood pressure control as opposed to pharmacologic intensity of RAAS blockade.
针对常染色体显性多囊肾病(ADPKD)早期阶段的HALT PKD试验表明,与标准控制相比,将收缩压强化控制在95 - 110 mmHg可使肾脏体积增长速度减慢14%。目前尚不清楚这一结果是由于在低血压组允许使用更高剂量药物从而对肾素 - 血管紧张素 - 醛固酮系统(RAAS)产生了更强的阻滞作用,还是由于血压本身较低所致。
在对HALT PKD研究A的这项二次分析中,我们根据初始剂量滴定期后使用的RAAS阻断药物的每日等效剂量中位数,将参与者分为高剂量组和低剂量组。使用线性混合模型,我们比较了两组之间总肾体积的百分比变化以及估计肾小球滤过率(eGFR)的斜率。我们还评估了随时间变化的剂量和随时间变化的血压参数对这些结果的影响。
在对年龄、性别、基因型和血压组进行调整后,高剂量组(n = 252)的总肾体积增加速度并不比低剂量组(n = 225)慢。两组中eGFR下降的慢性斜率相似。较高的随时间变化的收缩压与eGFR更陡峭的下降相关。
与RAAS阻滞的药物强度相比,强化血压控制可改善ADPKD的进展(通过eGFR下降和TKV增加来检测)。