Diabetes Care. 2018 May;41(5):917-928. doi: 10.2337/dci18-0007. Epub 2018 Mar 22.
This study updates previous estimates of the economic burden of diagnosed diabetes and quantifies the increased health resource use and lost productivity associated with diabetes in 2017.
We use a prevalence-based approach that combines the demographics of the U.S. population in 2017 with diabetes prevalence, epidemiological data, health care cost, and economic data into a Cost of Diabetes Model. Health resource use and associated medical costs are analyzed by age, sex, race/ethnicity, insurance coverage, medical condition, and health service category. Data sources include national surveys, Medicare standard analytical files, and one of the largest claims databases for the commercially insured population in the U.S.
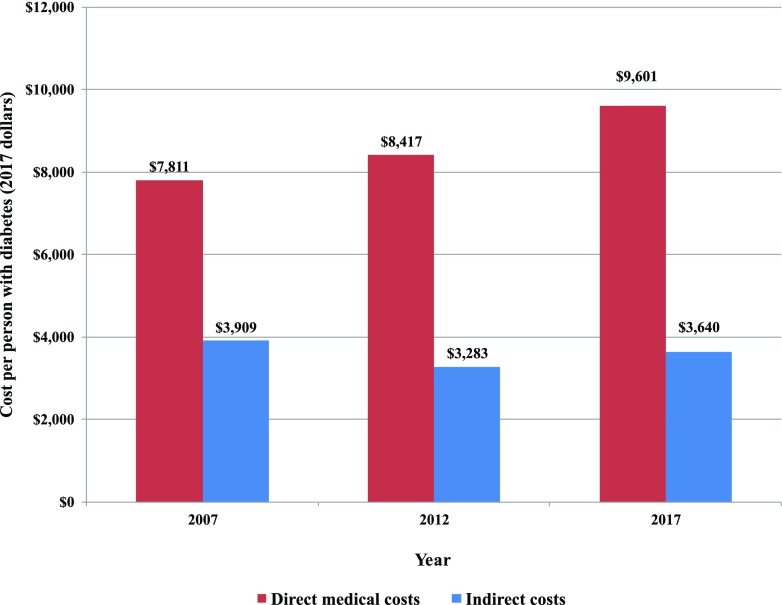
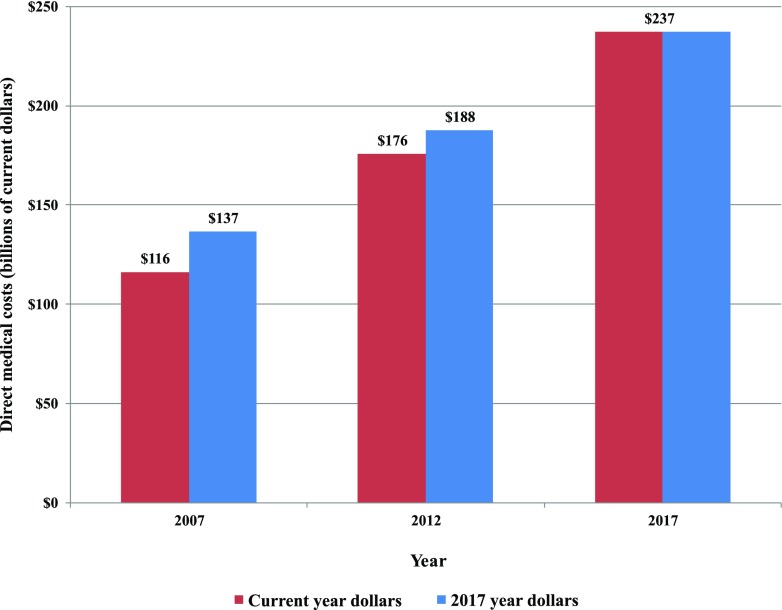
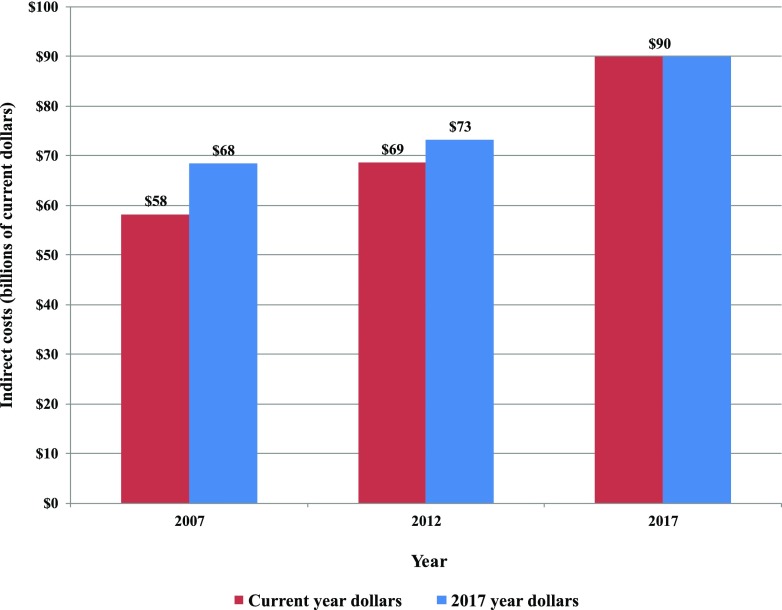
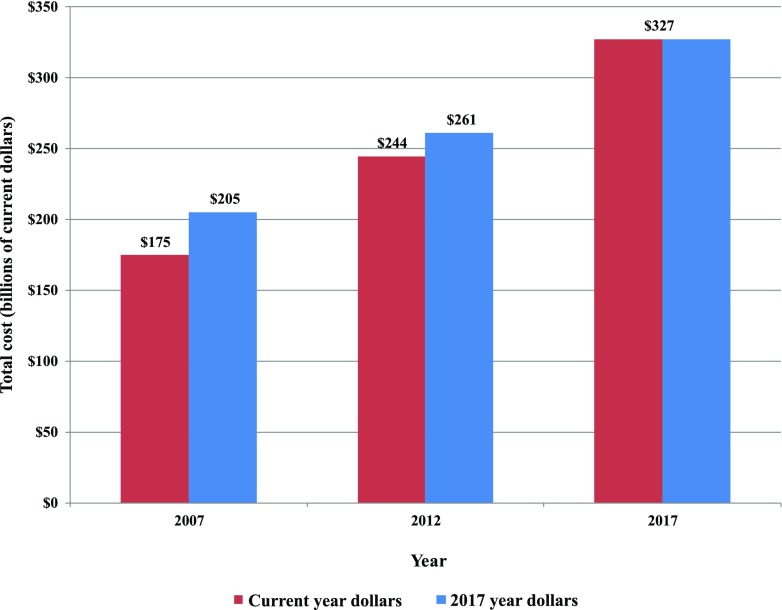
The total estimated cost of diagnosed diabetes in 2017 is $327 billion, including $237 billion in direct medical costs and $90 billion in reduced productivity. For the cost categories analyzed, care for people with diagnosed diabetes accounts for 1 in 4 health care dollars in the U.S., and more than half of that expenditure is directly attributable to diabetes. People with diagnosed diabetes incur average medical expenditures of ∼$16,750 per year, of which ∼$9,600 is attributed to diabetes. People with diagnosed diabetes, on average, have medical expenditures ∼2.3 times higher than what expenditures would be in the absence of diabetes. Indirect costs include increased absenteeism ($3.3 billion) and reduced productivity while at work ($26.9 billion) for the employed population, reduced productivity for those not in the labor force ($2.3 billion), inability to work because of disease-related disability ($37.5 billion), and lost productivity due to 277,000 premature deaths attributed to diabetes ($19.9 billion).
After adjusting for inflation, economic costs of diabetes increased by 26% from 2012 to 2017 due to the increased prevalence of diabetes and the increased cost per person with diabetes. The growth in diabetes prevalence and medical costs is primarily among the population aged 65 years and older, contributing to a growing economic cost to the Medicare program. The estimates in this article highlight the substantial financial burden that diabetes imposes on society, in addition to intangible costs from pain and suffering, resources from care provided by nonpaid caregivers, and costs associated with undiagnosed diabetes.
本研究更新了以往对确诊糖尿病经济负担的估计,并量化了 2017 年糖尿病导致的医疗资源使用增加和生产力损失。
我们采用基于患病率的方法,将 2017 年美国人口的人口统计学特征与糖尿病患病率、流行病学数据、医疗保健成本和经济数据结合到一个糖尿病成本模型中。按年龄、性别、种族/族裔、保险覆盖范围、医疗状况和卫生服务类别分析医疗资源使用和相关医疗费用。数据来源包括全国性调查、医疗保险标准分析文件以及美国商业保险人群中最大的索赔数据库之一。
2017 年确诊糖尿病的总估计费用为 3270 亿美元,其中 2370 亿美元为直接医疗费用,900 亿美元为生产力下降。在所分析的费用类别中,患有确诊糖尿病的人占美国医疗保健支出的 1/4,其中超过一半的支出直接归因于糖尿病。患有确诊糖尿病的人每年平均医疗支出约为 16750 美元,其中约 9600 美元归因于糖尿病。患有确诊糖尿病的人平均医疗支出是不存在糖尿病时的 2.3 倍。间接成本包括在职人群的旷工增加(33 亿美元)和工作时生产力下降(269 亿美元)、非劳动力人群的生产力下降(23 亿美元)、因疾病相关残疾而无法工作(375 亿美元)以及 277000 例归因于糖尿病的过早死亡导致的生产力下降(199 亿美元)。
经通胀调整后,2012 年至 2017 年,由于糖尿病患病率的增加和每人糖尿病成本的增加,糖尿病的经济成本增加了 26%。糖尿病患病率和医疗费用的增长主要发生在 65 岁及以上人群中,这导致医疗保险计划的经济成本不断增加。本文中的估计值除了强调糖尿病给社会带来的巨大经济负担外,还强调了痛苦和痛苦带来的无形成本、非付费护理人员提供的护理资源以及未确诊糖尿病带来的成本。