Battistella Marisa, Jandoc Racquel, Ng Jeremy Y, McArthur Eric, Garg Amit X
Department of Pharmacy, University Health Network, Toronto, Ontario, Canada.
Faculty of Pharmacy, University of Toronto, Ontario, Canada.
Can J Kidney Health Dis. 2018 Mar 13;5:2054358118760832. doi: 10.1177/2054358118760832. eCollection 2018.
Hemodialysis patients are at an increased risk of polypharmacy as they have the highest pill burden of all chronically ill patient populations, with an estimated average of 12 medications per day.
The aim of this study was to evaluate prescribing patterns of outpatient medications in patients receiving in-center hemodialysis. This was done to identify potential candidate medications for future quality improvement initiations to optimize prescribing.
We conducted a descriptive retrospective cross-sectional study in the province of Ontario, Canada, using several linked health care databases housed at the Institute for Clinical Evaluative Sciences (ICES).
We considered outpatient medications dispensed to patients eligible for the Ontario Drug Benefit program.
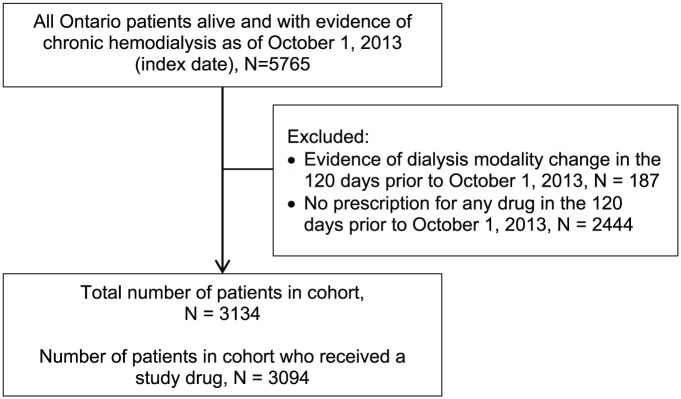
Patients were receiving chronic in-center hemodialysis at one of the 69 facilities in the province of Ontario, Canada as of October 1, 2013.
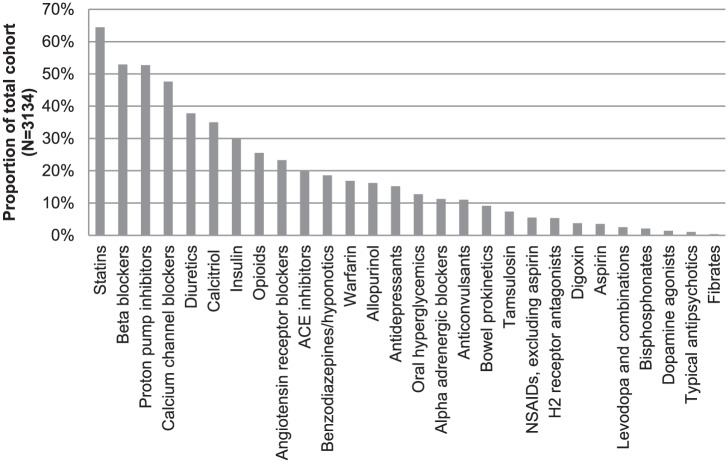
We assessed whether any of our 28 study medications of interest were recently dispensed (within the prior 120 days), the type of prescribing physician, and the associated medication costs. The 28 included medications of interest (ie, proton pump inhibitors, benzodiazepines) were selected because they may not have a true indication for dialysis patients and/or there are safety concerns with their use in this population. Results are presented as median (25th, 75th percentile).
We conducted this study at ICES according to a prespecified protocol approved by the Research Ethics Board at Sunnybrook Health Sciences Centre (Toronto, Ontario).
A total of 3094 patients on chronic in-center hemodialysis received a study drug of interest (age: 76.5 years [SD: 7.3]), 44% women). Patients were dispensed 11 (8, 14) unique medication products with more than two-thirds of patients dispensed 9 or more different medications. The median number of annual health care visits was 7 (3-15) with more than half the cohort receiving prescriptions from 3 or more specialists. The 10 most commonly dispensed study medications cost more than 3 million dollars in direct costs in 1 year.
Our study was also subjected to some limitations of health care databases.
Polypharmacy is frequent in in-center hemodialysis patients. To decrease polypharmacy and its associated negative outcomes, health care providers need to implement tools to optimize medication use and deprescribe medications that lack evidence for efficacy and safety in hemodialysis patients. Therefore, strategies to improve prescribing and discontinue ineffective medications warrant testing for better patient outcomes and reduced health care costs.
血液透析患者多重用药风险增加,因为在所有慢性病患者群体中他们的用药负担最重,估计平均每天服用12种药物。
本研究旨在评估接受中心血液透析患者的门诊用药处方模式。这样做是为了确定未来质量改进举措的潜在候选药物,以优化处方。
我们在加拿大安大略省进行了一项描述性回顾性横断面研究,使用了临床评估科学研究所(ICES)保存的多个相关医疗保健数据库。
我们考虑了发放给符合安大略药物福利计划资格患者的门诊药物。
截至2013年10月1日,患者在加拿大安大略省69家医疗机构之一接受慢性中心血液透析。
我们评估了我们感兴趣的28种研究药物中是否有任何一种最近(在过去120天内)被配药、开处方医生的类型以及相关药物成本。选择这28种感兴趣的药物(即质子泵抑制剂、苯二氮䓬类药物)是因为它们可能对透析患者没有真正的适应证,和/或在该人群中使用存在安全问题。结果以中位数(第25百分位数,第75百分位数)表示。
我们按照桑尼布鲁克健康科学中心(安大略省多伦多)研究伦理委员会批准的预先指定方案在ICES进行了这项研究。
共有3094名接受慢性中心血液透析的患者服用了一种感兴趣的研究药物(年龄:76.5岁[标准差:7.3],44%为女性)。患者配到了11种(8种,14种)不同的药物产品,超过三分之二的患者配到了9种或更多不同药物。每年医疗就诊的中位数次数为7次(3 - 15次),超过一半的队列患者从3名或更多专科医生处获得处方。10种最常配药的研究药物在1年中的直接成本超过300万美元。
我们的研究也受到医疗保健数据库的一些局限性的影响。
中心血液透析患者中多重用药很常见。为了减少多重用药及其相关负面结果,医疗保健提供者需要实施工具来优化药物使用,并停用在血液透析患者中缺乏疗效和安全性证据的药物。因此,改善处方和停用无效药物的策略值得进行测试,以实现更好的患者结局并降低医疗保健成本。