Kalmar A F, Allaert S, Pletinckx P, Maes J-W, Heerman J, Vos J J, Struys M M R F, Scheeren T W L
Department of Anesthesia and Critical Care Medicine, Maria Middelares Hospital, Buitenring Sint-Denijs 30, 9000, Ghent, Belgium.
Department of Anesthesiology, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands.
J Clin Monit Comput. 2018 Dec;32(6):969-976. doi: 10.1007/s10877-018-0126-3. Epub 2018 Mar 22.
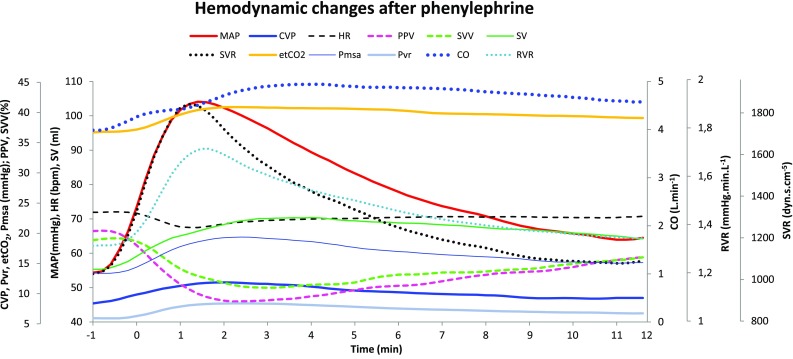
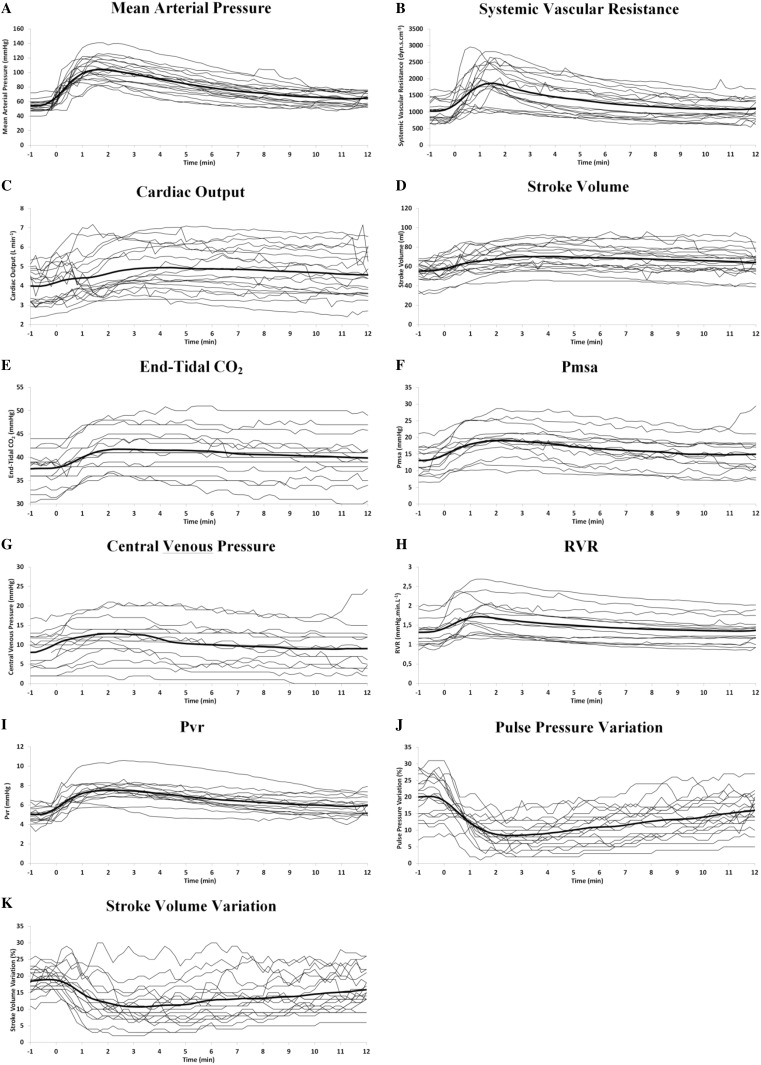
Induction of general anesthesia frequently induces arterial hypotension, which is often treated with a vasopressor, such as phenylephrine. As a pure α-agonist, phenylephrine is conventionally considered to solely induce arterial vasoconstriction and thus increase cardiac afterload but not cardiac preload. In specific circumstances, however, phenylephrine may also contribute to an increase in venous return and thus cardiac output (CO). The aim of this study is to describe the initial time course of the effects of phenylephrine on various hemodynamic variables and to evaluate the ability of advanced hemodynamic monitoring to quantify these changes through different hemodynamic variables. In 24 patients, after induction of anesthesia, during the period before surgical stimulus, phenylephrine 2 µg kg was administered when the MAP dropped below 80% of the awake state baseline value for > 3 min. The mean arterial blood pressure (MAP), heart rate (HR), end-tidal CO (EtCO), central venous pressure (CVP), stroke volume (SV), CO, pulse pressure variation (PPV), stroke volume variation (SVV) and systemic vascular resistance (SVR) were recorded continuously. The values at the moment before administration of phenylephrine and 5(T) and 10(T) min thereafter were compared. After phenylephrine, the mean(SD) MAP, SV, CO, CVP and EtCO increased by 34(13) mmHg, 11(9) mL, 1.02(0.74) L min, 3(2.6) mmHg and 4.0(1.6) mmHg at T respectively, while both dynamic preload variables decreased: PPV dropped from 20% at baseline to 9% at T and to 13% at T and SVV from 19 to 11 and 14%, respectively. Initially, the increase in MAP was perfectly aligned with the increase in SVR, until 150 s after the initial increase in MAP, when both curves started to dissociate. The dissociation of the evolution of MAP and SVR, together with the changes in PPV, CVP, EtCO and CO indicate that in patients with anesthesia-induced hypotension, phenylephrine increases the CO by virtue of an increase in cardiac preload.
全身麻醉诱导常常会引起动脉低血压,这种情况通常用血管升压药进行治疗,如去氧肾上腺素。作为一种纯α受体激动剂,传统上认为去氧肾上腺素仅能引起动脉血管收缩,从而增加心脏后负荷,但不会增加心脏前负荷。然而,在特定情况下,去氧肾上腺素也可能有助于增加静脉回心血量,进而增加心输出量(CO)。本研究的目的是描述去氧肾上腺素对各种血流动力学变量影响的初始时间进程,并评估先进血流动力学监测通过不同血流动力学变量量化这些变化的能力。在24例患者中,麻醉诱导后,在手术刺激前的时间段内,当平均动脉压(MAP)降至清醒状态基线值的80%以下超过3分钟时,给予2μg/kg的去氧肾上腺素。持续记录平均动脉血压(MAP)、心率(HR)、呼出二氧化碳浓度(EtCO)、中心静脉压(CVP)、每搏量(SV)、心输出量(CO)、脉压变异度(PPV)、每搏量变异度(SVV)和全身血管阻力(SVR)。比较给予去氧肾上腺素前即刻以及给药后5(T)分钟和10(T)分钟时的值。给予去氧肾上腺素后,在T时平均(标准差)MAP、SV、CO、CVP和EtCO分别增加了34(13)mmHg、11(9)mL、1.02(0.74)L/min、3(2.6)mmHg和4.0(1.6)mmHg,而两个动态前负荷变量均降低:PPV从基线时的20%降至T时的9%,再降至T时的13%,SVV从19%分别降至11%和14%。最初,MAP的升高与SVR的升高完全一致,直到MAP初始升高后150秒,此时两条曲线开始分离。MAP和SVR变化过程的分离,以及PPV、CVP、EtCO和CO的变化表明,在麻醉诱导性低血压患者中,去氧肾上腺素通过增加心脏前负荷来增加心输出量。