Zhu Li, Li Hanbin, Chan Phyllis, Eley Timothy, Gandhi Yash, Bifano Marc, Osawa Mayu, Ueno Takayo, Hughes Eric, AbuTarif Malaz, Bertz Richard, Garimella Tushar
Bristol-Myers Squibb Research and Development, Lawrenceville, NJ, USA.
Quantitative Solutions, Menlo Park, CA, USA.
Infect Dis Ther. 2018 Jun;7(2):261-275. doi: 10.1007/s40121-018-0197-y. Epub 2018 Mar 27.
Asunaprevir (ASV) is a potent, pangenotypic, twice-daily hepatitis C virus (HCV) NS3 inhibitor indicated for the treatment of chronic HCV infection.
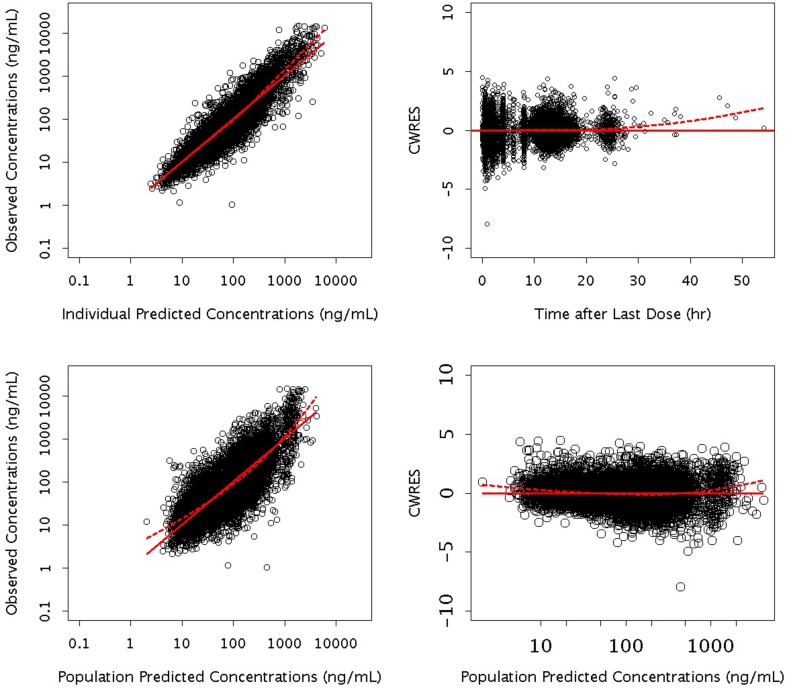
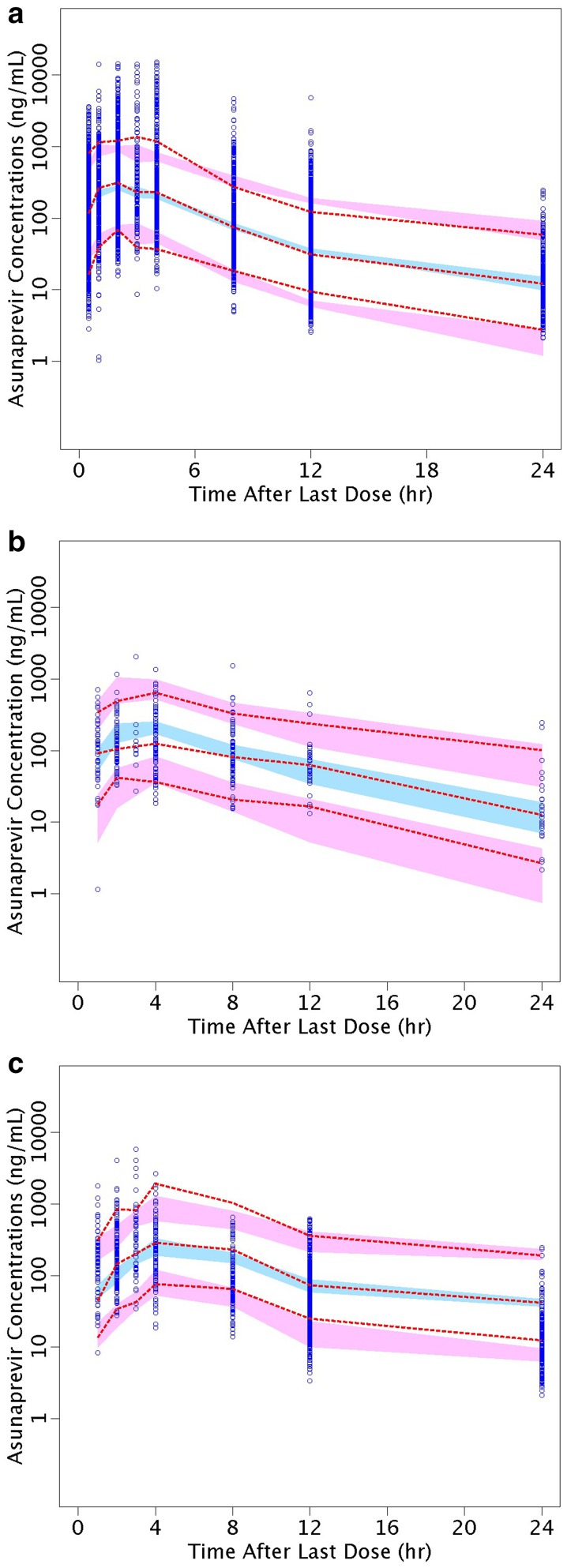
A population pharmacokinetic (PPK) model was developed using pooled ASV concentration data from 1239 HCV-infected subjects who received ASV either as part of the DUAL regimen with daclatasvir or as part of the QUAD regimen with daclatasvir and peg-interferon/ribavirin.
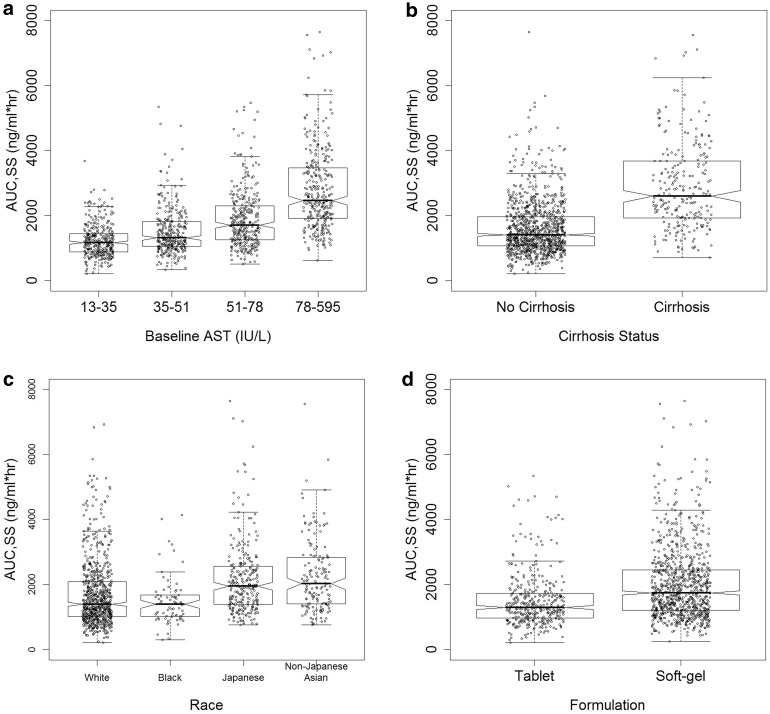
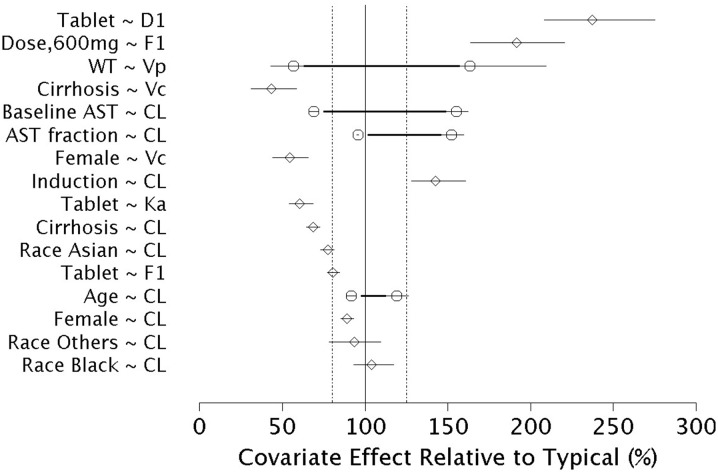
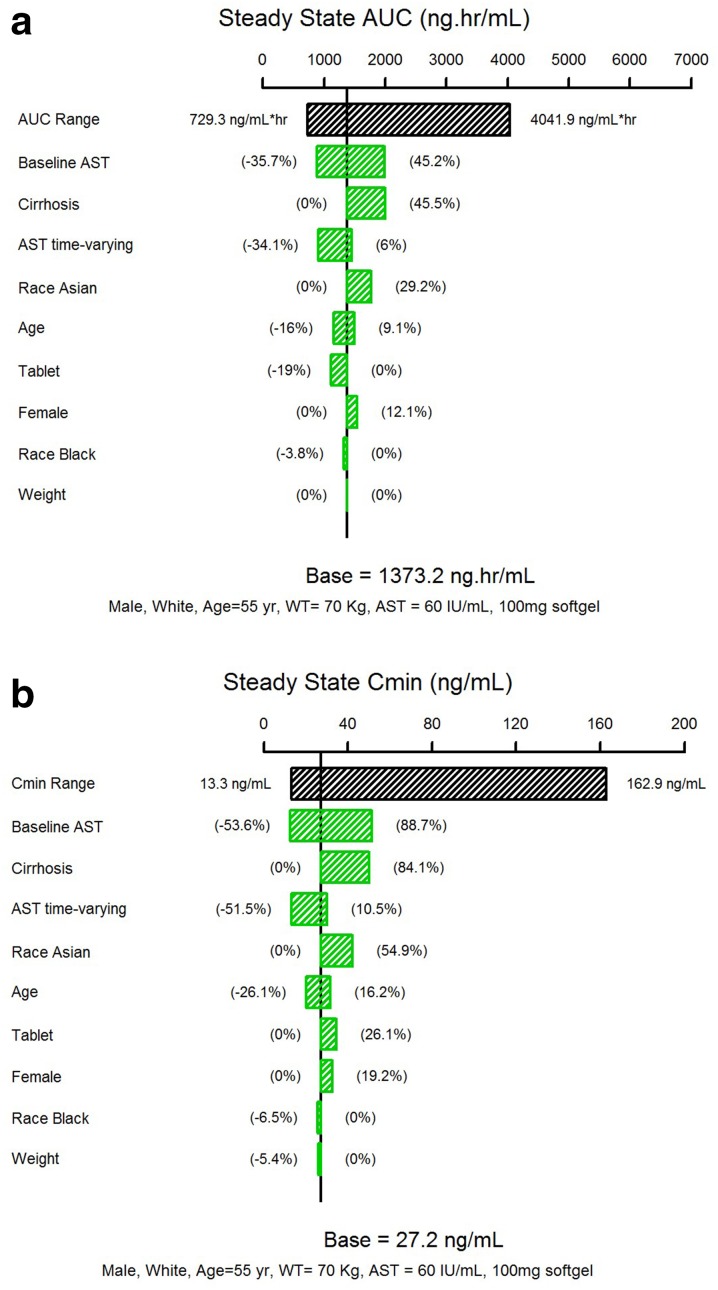
A two-compartment model with first-order elimination from the central compartment, an induction effect on clearance, and an absorption model consisted of zero-order release followed by first-order absorption adequately described ASV PK after oral administration. A typical value for ASV clearance (CL/F) was 50.8 L/h, increasing by 43% after 2 days to a CL/F of 72.5 L/h at steady-state, likely due to auto-induction of cytochrome P450 3A4 (CYP3A4). Factors indicative of hepatic function were identified as key influential covariates on ASV exposures. Subjects with cirrhosis had an 84% increase in ASV area under the concentration time curve (AUC) and subjects with baseline aspartate aminotransferase (AST) above 78 IU/L had a 58% increase in area under the concentration time curve (AUC). Asians subjects had a 46% higher steady-state AUC relative to White/Caucasian subjects. Other significant covariates were formulation, age, and gender.
The current PPK model provided a parsimonious description of ASV concentration data in HCV-infected subjects. Key covariates identified in the model help explain the observed variability in ASV exposures and may guide clinical use of the drug.
Bristol-Myers Squibb.
asunaprevir(ASV)是一种强效、泛基因型、每日两次给药的丙型肝炎病毒(HCV)NS3抑制剂,用于治疗慢性HCV感染。
利用来自1239名HCV感染受试者的ASV浓度汇总数据建立群体药代动力学(PPK)模型,这些受试者接受ASV治疗,ASV作为与daclatasvir联合治疗方案(DUAL方案)的一部分,或作为与daclatasvir及聚乙二醇干扰素/利巴韦林联合治疗方案(QUAD方案)的一部分。
一个具有从中央室一级消除、清除率诱导效应以及由零级释放后接一级吸收组成的吸收模型的二室模型,充分描述了口服给药后ASV的药代动力学特征。ASV清除率(CL/F)的典型值为50.8 L/h,在2天后增加43%,在稳态时CL/F达到72.5 L/h,这可能是由于细胞色素P450 3A4(CYP3A4)的自身诱导作用所致。肝功能指标被确定为对ASV暴露有关键影响的协变量。肝硬化患者的ASV浓度-时间曲线下面积(AUC)增加84%,基线天冬氨酸氨基转移酶(AST)高于78 IU/L的患者的浓度-时间曲线下面积(AUC)增加58%。亚洲受试者的稳态AUC相对于白人/高加索受试者高46%。其他显著的协变量包括剂型、年龄和性别。
当前的PPK模型对HCV感染受试者的ASV浓度数据提供了简洁的描述。模型中确定的关键协变量有助于解释观察到的ASV暴露变异性,并可能指导该药物的临床应用。
百时美施贵宝公司。