Osses Daniël F, Alberts Arnout R, Bausch Gonny C F, Roobol Monique J
Department of Urology, Erasmus University Medical Center, Rotterdam, The Netherlands.
STAR-SHL Medical Diagnostic Center, GP laboratory, Rotterdam, The Netherlands.
Transl Androl Urol. 2018 Feb;7(1):27-33. doi: 10.21037/tau.2017.12.11.
According to their guidelines, Dutch general practitioners (GPs) refer men with prostate-specific antigen (PSA) level ≥3.0 ng/mL to the urologist for risk-based patient selection for prostate biopsy using the Rotterdam Prostate Cancer Risk Calculator (RPCRC). Use of the RPCRC in primary care could optimize the diagnostic pathway even further by reducing unnecessary referrals. To investigate this, we calculated the risk and assessed the rate of men referred to the urologist with PSA level ≥3.0 ng/mL by implementing the RPCRC in a primary health care setting.
In January 2014, an exploratory study was initiated in collaboration with the primary health care facility of the GP laboratory in Rotterdam. GPs were given the possibility to refer men with a suspicion of prostate cancer (PCa) or a screening wish to this primary care facility (STAR-SHL) where further assessment was performed by specially trained personnel. Risk-based advice on referral to the urologist was given to the GP on the basis of the RPCRC results. If requested, advice on the treatment of lower urinary tract symptoms (LUTS) was provided. All men signed informed consent.
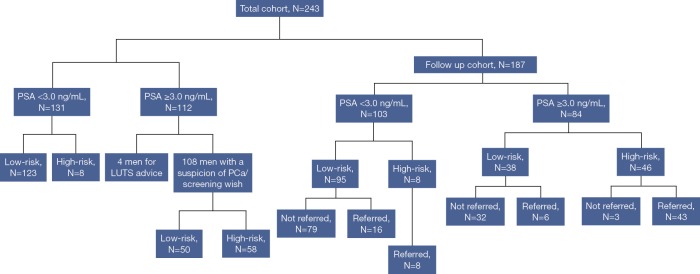
Between January 2014 and September 2017, a total of 243 men, median age 64 [interquartile range (IQR), 57-70] years were referred for a consultation at the primary care facility. Of the 108 men with PSA level ≥3.0 ng/mL and a referral related to PCa, GPs were advised to refer 58 men to the urologist (54%). Of the men with available follow-up (FU) data [n=187, median FU, 16 (IQR, 9-25) months] 54 men were considered high-risk (i.e., had an elevated risk of PCa as calculated by the RPCRC). Of these men, 51 (94%) were actually referred to secondary care by their GP, and so far 38 men underwent biopsy. PCa was detected in 30 men [47% had Gleason score (GS) ≥3+4 PCa], translating to an overall positive predictive value (PPV) of 79%. Within the available FU time, 2 out of 38 (5%) men with PSA level ≥3.0 ng/mL which were considered low-risk have been diagnosed with GS 3+3 PCa.
Risk-stratification with the RPCRC in a primary health care setting could prevent almost half of referrals of men with PSA level ≥3.0 ng/mL to the urologist. In more than three-quarters of men referred for prostate biopsy, the suspicion of PCa was confirmed and almost half of men had clinically significant PCa (GS ≥3+4 PCa). These data show a huge potential for multivariable risk-stratification in primary care.
根据其指南,荷兰全科医生(GP)会将前列腺特异性抗原(PSA)水平≥3.0 ng/mL的男性转介给泌尿科医生,以便使用鹿特丹前列腺癌风险计算器(RPCRC)进行基于风险的前列腺活检患者选择。在初级保健中使用RPCRC可以通过减少不必要的转诊进一步优化诊断途径。为了对此进行研究,我们在初级卫生保健机构中实施RPCRC,计算了PSA水平≥3.0 ng/mL的男性被转介给泌尿科医生的风险并评估了这一比例。
2014年1月,与鹿特丹GP实验室的初级卫生保健机构合作开展了一项探索性研究。GP们可以将怀疑患有前列腺癌(PCa)或有筛查意愿的男性转介到该初级保健机构(STAR-SHL),由经过专门培训的人员进行进一步评估。根据RPCRC结果为GP提供关于转介到泌尿科医生的基于风险的建议。如果有要求,还会提供关于下尿路症状(LUTS)治疗的建议。所有男性均签署了知情同意书。
2014年1月至2017年9月期间,共有243名男性,中位年龄64岁[四分位间距(IQR),57 - 70岁]被转介到初级保健机构进行咨询。在108名PSA水平≥3.0 ng/mL且转诊与PCa相关的男性中,建议GP将58名男性转介给泌尿科医生(54%)。在有可用随访(FU)数据的男性中[n = 187,中位FU时间,16(IQR,9 - 25)个月],54名男性被认为是高风险(即根据RPCRC计算出患PCa的风险升高)。在这些男性中,51名(94%)实际上被其GP转介到二级保健机构,到目前为止38名男性接受了活检。在30名男性中检测到PCa[47%的患者Gleason评分(GS)≥3 + 4 PCa],总体阳性预测值(PPV)为79%。在可用的FU时间内,38名被认为是低风险的PSA水平≥3.0 ng/mL的男性中有2名(5%)被诊断为GS 3 + 3 PCa。
在初级卫生保健机构中使用RPCRC进行风险分层可以避免几乎一半PSA水平≥3.0 ng/mL的男性被转介给泌尿科医生。在超过四分之三被转介进行前列腺活检的男性中,对PCa的怀疑得到了证实,并且几乎一半的男性患有具有临床意义的PCa(GS≥3 + 4 PCa)。这些数据表明在初级保健中进行多变量风险分层具有巨大潜力。