Dolan Ross D, McSorley Stephen T, Horgan Paul G, McMillan Donald C
Academic Unit of Surgery, School of Medicine, University of Glasgow, Glasgow Royal Infirmary, Glasgow, UK.
Medicine (Baltimore). 2018 Mar;97(13):e0185. doi: 10.1097/MD.0000000000010185.
Prognosis in colon cancer is based on pathological criteria including TNM staging. However, there are deficiencies in this approach, and the lymph node ratio (LNR) has been proposed to improve the prediction of outcomes. LNR is dependent on optimal retrieval of lymph nodes-lymph node count (LNC). Recent studies have suggested that an elevated preoperative systemic inflammatory response (SIR) was associated with a lower LNC and a higher LNR. However, there are a number of potential confounding factors. The aim of the present study was to examine, in detail, these relationships in a large cohort of patients.A prospectively maintained database of all patients undergoing colon cancer resection in our institution was examined. The SIR was measured by a number of inflammatory markers and their scores: modified Glasgow Prognostic Score (mGPS) (C-reactive protein/albumin), neutrophil lymphocyte ratio (NLR), platelet lymphocyte ratio (PLR), and lymphocyte monocyte ratio (LMR) using standard thresholds. The relationships between LNC and LNR, and clinicopathological characteristics (including the mGPS, NLR, PLR, and LMR) were examined using chi-square test for trend and binary logistic regression analysis, where appropriate.Of the 896 patients included in the study, 418 (47%) were male, the median LNC was 17 (1-71), and the median LNR in node positive disease was 0.16 (0.03-1). On multivariate analysis, there was a significant independent relationship between an elevated LNC (≥12) and laparoscopic surgery (P < .001), right-sided tumors (P < .001), later date of resection (2007-2016) (P < .001), T stage (P < .001), and venous invasion (P < .001). In those patients with a LNC ≥12 and node-positive disease (n = 272), on multivariate analysis, there was a significant relationship between an elevated LNR (≥0.25), and T stage (P < .01) and differentiation (P < .05). Finally, in patients with node-positive disease who had surgery later (2007-2016), LNR was directly superior to N stage for both cancer-specific survival (LNR: hazard ratio [HR] 2.62, 95% confidence interval [CI] 1.25-5.52, P = .011) and overall survival (LNR: HR 2.02, 95% CI 1.12-3.68, P = .022).Neither LNC nor LNR was associated with markers of the SIR; however, LNC and LNR were directly associated. In high-quality surgical and pathological practice, LNR had superior prognostic value compared with N stage in patients undergoing surgery for colon cancer.
结肠癌的预后基于包括TNM分期在内的病理标准。然而,这种方法存在不足之处,因此有人提出用淋巴结比率(LNR)来改善对预后的预测。LNR取决于淋巴结的最佳获取情况,即淋巴结计数(LNC)。最近的研究表明,术前全身炎症反应(SIR)升高与较低的LNC和较高的LNR相关。然而,存在许多潜在的混杂因素。本研究的目的是在一大群患者中详细研究这些关系。
我们检查了本机构所有接受结肠癌切除术患者的前瞻性维护数据库。通过多种炎症标志物及其评分来测量SIR:改良格拉斯哥预后评分(mGPS)(C反应蛋白/白蛋白)、中性粒细胞淋巴细胞比率(NLR)、血小板淋巴细胞比率(PLR)和淋巴细胞单核细胞比率(LMR),使用标准阈值。在适当情况下,使用趋势卡方检验和二元逻辑回归分析来研究LNC与LNR以及临床病理特征(包括mGPS、NLR、PLR和LMR)之间的关系。
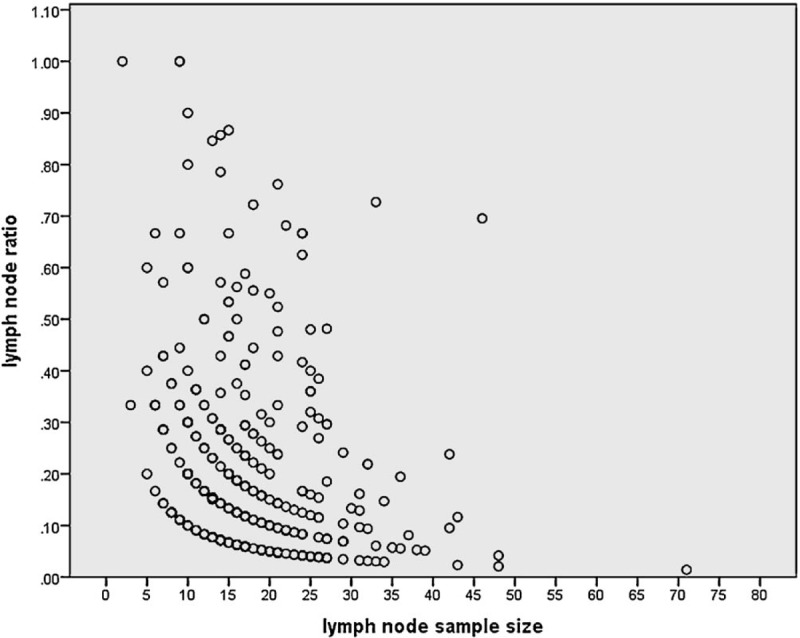
在纳入研究的896例患者中,418例(47%)为男性,LNC中位数为17(1 - 71),淋巴结阳性疾病患者的LNR中位数为0.16(0.03 - 1)。多因素分析显示,LNC升高(≥12)与腹腔镜手术(P <.001)、右侧肿瘤(P <.001)、较晚的切除日期(2007 - 2016年)(P <.001)、T分期(P <.001)和静脉侵犯(P <.001)之间存在显著的独立关系。在LNC≥12且淋巴结阳性的患者(n = 272)中,多因素分析显示,LNR升高(≥0.25)与T分期(P <.01)和分化程度(P <.05)之间存在显著关系。最后,在2007 - 2016年较晚接受手术的淋巴结阳性疾病患者中,LNR在癌症特异性生存(LNR:风险比[HR] 2.62,95%置信区间[CI] 1.25 - 5.52,P =.011)和总生存(LNR:HR 2.02,95% CI 1.12 - 3.68,P =.022)方面均直接优于N分期。
LNC和LNR均与SIR的标志物无关;然而,LNC和LNR直接相关。在高质量的外科手术和病理实践中,对于接受结肠癌手术的患者,LNR相比N分期具有更好的预后价值。