Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, MN 55905, United States.
Department of Medicine, Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok 10400, Thailand.
World J Gastroenterol. 2018 Mar 28;24(12):1321-1331. doi: 10.3748/wjg.v24.i12.1321.
To assess the performance of BALAD, BALAD-2 and their component biomarkers in predicting outcome of hepatocellular carcinoma (HCC) patients after liver transplant.
BALAD score and BALAD-2 class are derived from bilirubin, albumin, alpha-fetoprotein (AFP), Lens culinaris agglutinin-reactive AFP (AFP-L3), and des-gamma-carboxyprothrombin (DCP). Pre-transplant AFP, AFP-L3 and DCP were measured in 113 patients transplanted for HCC from 2000 to 2008. Hazard ratios (HR) for recurrence and death were calculated. Univariate and multivariate regression analyses were conducted. C-statistics were used to compare biomarker-based to predictive models.
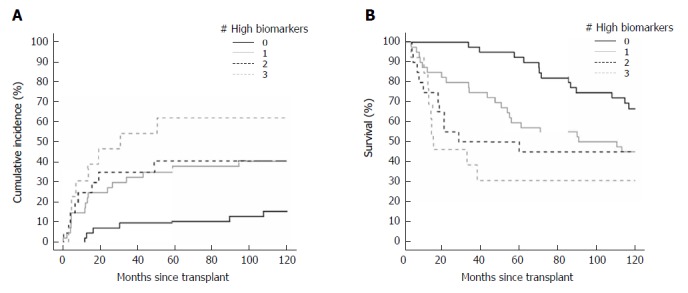
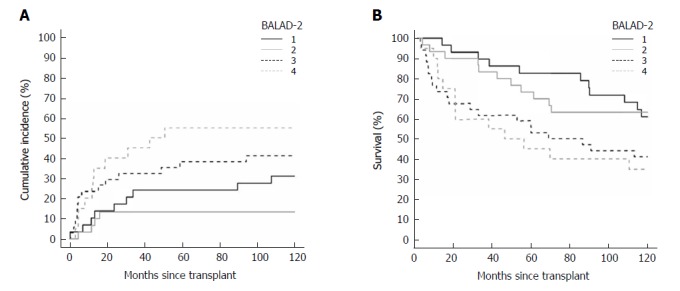
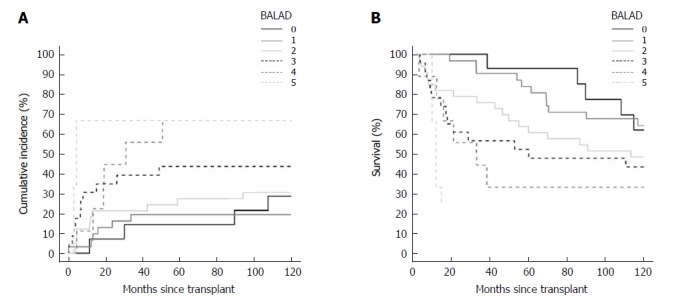
During a median follow-up of 12.2 years, 38 patients recurred and 87 died. The HRs for recurrence in patients with elevated AFP, AFP-L3, and DCP defined by BALAD cut-off values were 2.42 (1.18-5.00), 1.86 (0.98-3.52), and 2.83 (1.42-5.61), respectively. For BALAD, the HRs for recurrence and death per unit increased score were 1.48 (1.15-1.91) and 1.59 (1.28-1.97). For BALAD-2, the HRs for recurrence and death per unit increased class were 1.45 (1.06-1.98) and 1.38 (1.09-1.76). For recurrence prediction, the combination of three biomarkers had the highest c-statistic of 0.66 vs. 0.64, 0.61, 0.53, and 0.53 for BALAD, BALAD-2, Milan, and UCSF, respectively. Similarly, for death prediction, the combination of three biomarkers had the highest c-statistic of 0.66 0.65, 0.61, 0.52, and 0.50 for BALAD, BALAD-2, Milan, and UCSF. A new model combining biomarkers with tumor size at the time of transplant (S-LAD) demonstrated the highest predictive capability with c-statistics of 0.71 and 0.69 for recurrence and death.
BALAD and BALAD-2 are valid in transplant HCC patients, but less predictive than the three biomarkers in combination or the three biomarkers in combination with maximal tumor diameter (S-LAD).
评估 BALAD、BALAD-2 及其组成生物标志物在预测肝癌(HCC)患者肝移植后结局中的表现。
BALAD 评分和 BALAD-2 分级由胆红素、白蛋白、甲胎蛋白(AFP)、扁豆凝集素反应性 AFP(AFP-L3)和去γ-羧基凝血酶原(DCP)组成。2000 年至 2008 年间,对 113 例因 HCC 接受肝移植的患者进行了移植前 AFP、AFP-L3 和 DCP 的检测。计算了复发和死亡的风险比(HR)。进行了单变量和多变量回归分析。C 统计量用于比较基于生物标志物的预测模型。
在中位随访 12.2 年期间,38 例患者复发,87 例患者死亡。BALAD 截断值定义的 AFP、AFP-L3 和 DCP 升高患者的复发 HR 分别为 2.42(1.18-5.00)、1.86(0.98-3.52)和 2.83(1.42-5.61)。对于 BALAD,每增加一个单位的复发和死亡 HR 分别为 1.48(1.15-1.91)和 1.59(1.28-1.97)。对于 BALAD-2,每增加一个单位的复发和死亡 HR 分别为 1.45(1.06-1.98)和 1.38(1.09-1.76)。对于复发预测,三种生物标志物的组合具有最高的 C 统计量为 0.66,优于 BALAD、BALAD-2、米兰和 UCSF 的 0.64、0.61、0.53 和 0.53。同样,对于死亡预测,三种生物标志物的组合具有最高的 C 统计量为 0.66,优于 BALAD、BALAD-2、米兰和 UCSF 的 0.65、0.61、0.52 和 0.50。一个结合移植时肿瘤大小的新模型(S-LAD)具有最高的预测能力,复发和死亡的 C 统计量分别为 0.71 和 0.69。
BALAD 和 BALAD-2 在移植 HCC 患者中是有效的,但预测能力低于三种生物标志物的组合或三种生物标志物与最大肿瘤直径(S-LAD)的组合。