Department of Gastroenterological Surgery, Dokkyo Medical University, Tochigi 321-0293, Japan.
Department of Diagnostic Pathology, Dokkyo Medical University, Tochigi 321-0293, Japan.
World J Gastroenterol. 2018 Mar 28;24(12):1332-1342. doi: 10.3748/wjg.v24.i12.1332.
To evaluate the usefulness of frozen section diagnosis (FSD) of bile duct margins during surgery for extrahepatic cholangiocarcinoma (CCA).
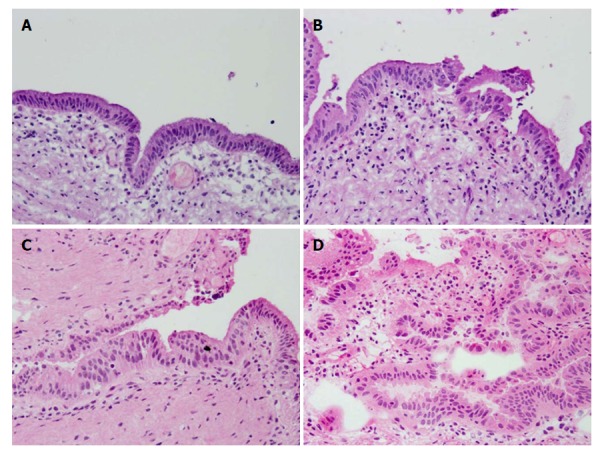
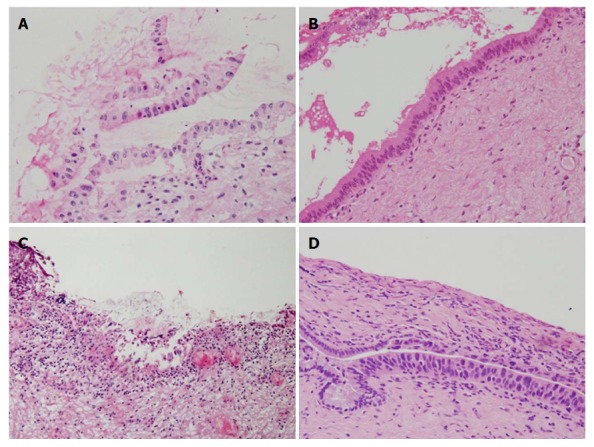
We retrospectively analyzed 74 consecutive patients who underwent surgery for extrahepatic CCA from 2012 to 2017, during which FSD of bile duct margins was performed. They consisted of 40 distant and 34 perihilar CCAs (45 and 55 bile duct margins, respectively). The diagnosis was classified into three categories: negative, borderline (biliary intraepithelial neoplasia-1 and 2, and indefinite for neoplasia), or positive. FSD in the epithelial layer, subepithelial layer, and total layer was compared with corresponding permanent section diagnosis (PSD) postoperatively. Then, association between FSD and local recurrence was analyzed with special reference to borderline.
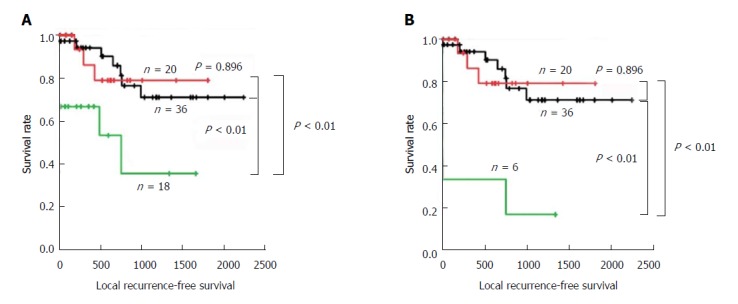
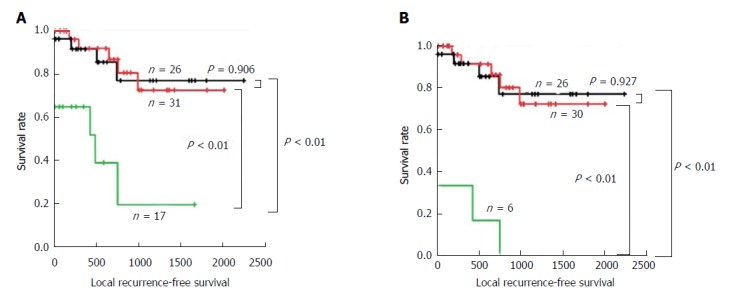
Analysis of 100 duct margins revealed that concordance rate between FSD and PSD was 68.0% in the total layer, 69.0% in the epithelial layer, and 98.0% in the subepithelial layer. The extent of remaining biliary epithelium was comparable between FSD and PSD, and more than half of the margins lost > 50% of the entire epithelium, suggesting low quality of the samples. In FSD, the rate of negative margins decreased and that of borderline and positive margins increased according to the extent of the remaining epithelium. Diagnostic discordance between FSD and PSD was observed in 31 epithelial layers and two subepithelial layers. Alteration from borderline to negative was the most frequent (20 of the 31 epithelial layers). Patients with positive margin in the total and epithelial layers by FSD demonstrated a significantly worse local recurrence-free survival (RFS) compared with patients with borderline and negative margins, which revealed comparable local RFS. Patients with borderline and negative margins in the epithelial layer by PSD also revealed comparable local RFS. These results suggested that epithelial borderline might be regarded substantially as negative. When classifying the status of the epithelial layer either as negative or positive, concordance rates between FSD and PSD in the total, epithelial, and subepithelial layers were 95.0%, 93.0%, and 98.0%, respectively.
During intraoperative assessment of bile duct margin, borderline in the epithelial layer can be substantially regarded as negative, under which condition FSD is comparable to PSD.
评估冰冻切片诊断(FSD)在肝外胆管癌(CCA)手术中胆管切缘的作用。
我们回顾性分析了 2012 年至 2017 年期间连续接受手术治疗的 74 例肝外 CCA 患者的资料,这些患者均接受了 FSD 检查。其中,40 例为远端 CCA,34 例为肝门部 CCA(分别有 45 个和 55 个胆管切缘)。诊断分为三类:阴性、交界性(胆管上皮内瘤变 1 级和 2 级和不确定为肿瘤)或阳性。比较了冰冻切片上皮层、黏膜下层和全层与术后石蜡切片诊断(PSD)的一致性。然后,特别参考交界性病变,分析了 FSD 与局部复发的关系。
对 100 个胆管切缘的分析表明,FSD 和 PSD 在全层的一致性率为 68.0%,在上皮层为 69.0%,在黏膜下层为 98.0%。FSD 和 PSD 检测的胆管上皮残留范围相当,超过一半的切缘失去了>50%的整个上皮,提示标本质量较差。在 FSD 中,根据残留上皮的范围,阴性切缘的比例降低,交界性和阳性切缘的比例增加。在 31 个上皮层和 2 个黏膜下层发现 FSD 与 PSD 之间的诊断不一致。从交界性改变为阴性是最常见的(31 个上皮层中有 20 个)。FSD 总切缘和上皮层阳性的患者局部无复发生存率(RFS)明显差于交界性和阴性切缘的患者,其局部 RFS 无差异。PSD 上皮层为交界性和阴性的患者局部 RFS 也无差异。这些结果表明,上皮交界性可被视为实质性的阴性。当将上皮层的状态分类为阴性或阳性时,FSD 和 PSD 在全层、上皮层和黏膜下层的一致性率分别为 95.0%、93.0%和 98.0%。
在胆管切缘的术中评估中,上皮层的交界性可被视为实质性的阴性,在此条件下,FSD 与 PSD 相当。