Academic Urology Group, Department of Surgery, University of Cambridge, Cambridge, UK.
Department of Urology, Addenbrooke's Hospital, Cambridge University Hospitals NHS Foundation Trust, Cambridge, UK.
BJU Int. 2018 Oct;122(4):599-609. doi: 10.1111/bju.14217. Epub 2018 Apr 20.
To describe the temporal trends in nephrectomy practice and outcomes for English patients with renal cell carcinoma (RCC).
Adult RCC nephrectomy patients treated between 2000 and 2010 were identified in the National Cancer Data Repository and Hospital Episode Statistics, and followed-up until date of death or 31 December 2015 (n = 30 763). We estimated the annual frequency for each nephrectomy type, the hospital and surgeon numbers and their case volumes. We analysed short-term surgical outcomes, as well as 1- and 5-year relative survivals.
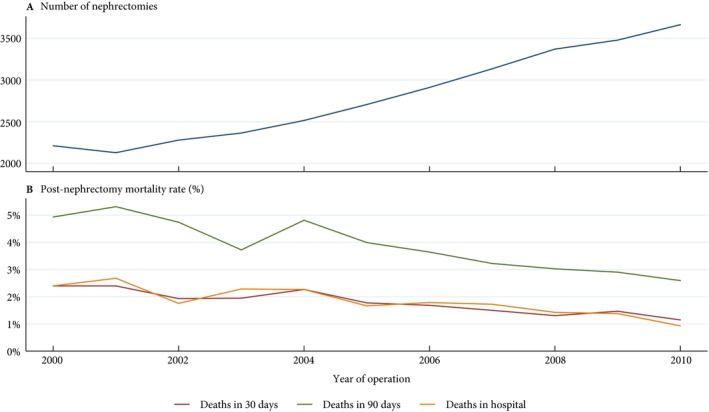
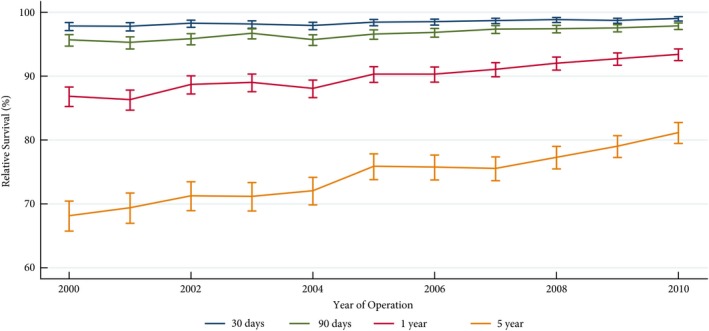
Annual RCC nephrectomy number increased by 66% during the study period. Hospital number decreased by 24%, whilst the median annual hospital volume increased from 10 to 23 (P < 0.01). Surgeon number increased by 27% (P < 0.01), doubling the median consultant number per hospital. The proportion of minimally invasive surgery (MIS) nephrectomies rose from 1% to 46%, whilst the proportion of nephron-sparing surgeries (NSS) increased from 5% to 16%, with 29% of all T1 disease treated with partial nephrectomy in 2010 (P < 0.01). The 30-day mortality rate halved from 2.4% to 1.1% and 90-day mortality decreased from 4.9% to 2.6% (P < 0.01). The 1-year relative survival rate increased from 86.9% to 93.4%, whilst the 5-year relative survival rate rose from 68.2% to 81.2% (P < 0.01). Improvements were most notable in patients aged ≥65 years and those with T3 and T4 disease.
Surgical RCC management has changed considerably with nephrectomy centralisation and increased NSS and MIS. In parallel, we observed significant improvements in short- and long-term survival particularly for elderly patients and those with locally advanced disease.
描述英国肾细胞癌(RCC)患者肾切除术实践和结果的时间趋势。
在国家癌症数据库和医院病例统计中确定了 2000 年至 2010 年间接受治疗的成年 RCC 肾切除术患者,并随访至死亡或 2015 年 12 月 31 日(n = 30763)。我们估计了每种肾切除术类型的年度频率、医院和外科医生数量及其病例量。我们分析了短期手术结果以及 1 年和 5 年相对生存率。
研究期间,RCC 肾切除术的年例数增加了 66%。医院数量减少了 24%,而中位数年度医院容量从 10 增加到 23(P < 0.01)。外科医生数量增加了 27%(P < 0.01),使中位数每位医院顾问的数量翻了一番。微创手术(MIS)肾切除术的比例从 1%上升到 46%,同时保肾手术(NSS)的比例从 5%上升到 16%,2010 年所有 T1 疾病中有 29%采用部分肾切除术治疗(P < 0.01)。30 天死亡率从 2.4%降至 1.1%,90 天死亡率从 4.9%降至 2.6%(P < 0.01)。1 年相对生存率从 86.9%上升到 93.4%,5 年相对生存率从 68.2%上升到 81.2%(P < 0.01)。在≥65 岁的患者和 T3 和 T4 疾病患者中,改善最为显著。
肾切除术的集中化以及 NSS 和 MIS 的增加导致了 RCC 手术管理的重大变化。与此同时,我们观察到短期和长期生存率的显著提高,特别是在老年患者和局部晚期疾病患者中。