Molecular Imaging Program, National Cancer Institute, NIH, Bethesda, Maryland, USA.
Clinical Research Directorate/Clinical Monitoring Research Program, Leidos Biomedical Research, Inc., Frederick National Laboratory for Cancer Research, Frederick, Maryland, 21702.
J Magn Reson Imaging. 2018 Nov;48(5):1326-1335. doi: 10.1002/jmri.26025. Epub 2018 Mar 31.
Prostate Imaging-Reporting and Data System v. 2 (PI-RADSv2) provides standardized nomenclature for interpretation of prostate multiparametric MRI (mpMRI). Inclusion of additional features for categorization may provide benefit to stratification of disease.
To prospectively compare PI-RADSv2 to a qualitative in-house system for detecting prostate cancer on mpMRI.
Prospective.
In all, 338 patients who underwent mpMRI May 2015-May 2016, with subsequent MRI/transrectal ultrasound fusion-guided biopsy.
3T mpMRI (T W, diffusion-weighted [DW], apparent diffusion coefficient [ADC] map, b-2000 DWI acquisition, and dynamic contrast-enhanced [DCE] MRI).
One genitourinary radiologist prospectively read mpMRIs using both in-house and PI-RADSv2 5-category systems.
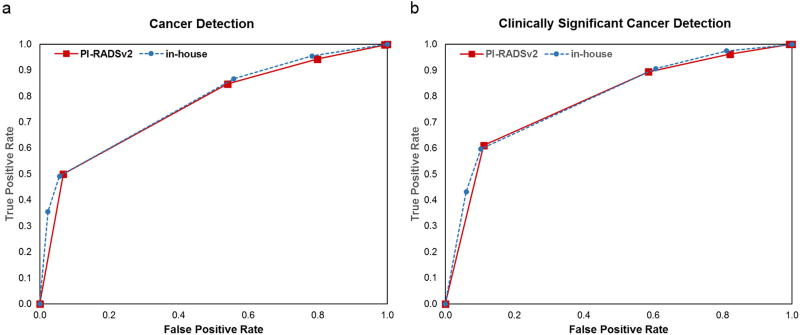
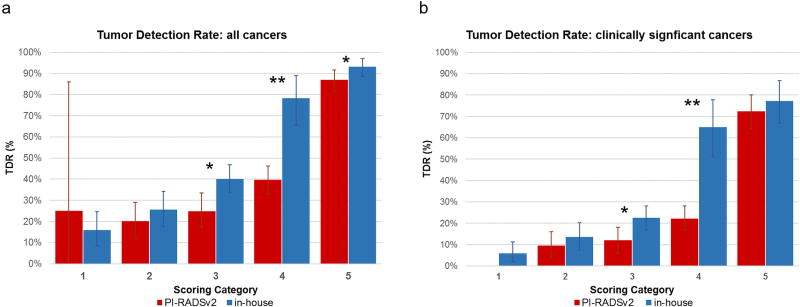
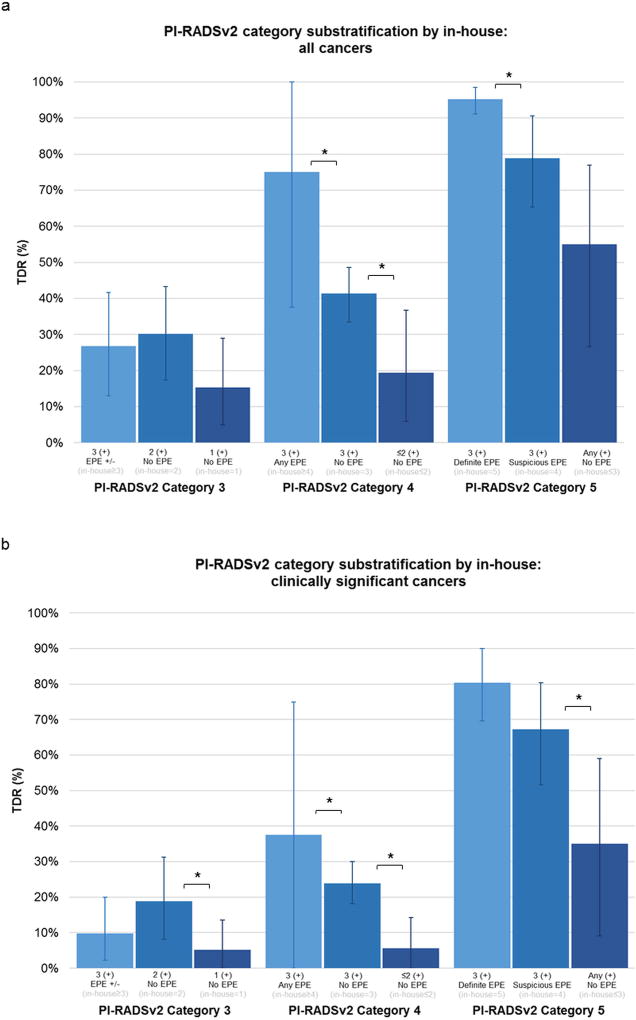
In lesion-based analysis, overall and clinically significant (CS) tumor detection rates (TDR) were calculated for all PI-RADSv2 and in-house categories. The ability of each scoring system to detect cancer was assessed by area under receiver operator characteristic curve (AUC). Within each PI-RADSv2 category, lesions were further stratified by their in-house categories to determine if TDRs can be increased by combining features of both systems.
In 338 patients (median prostate-specific antigen [PSA] 6.5 [0.6-113.6] ng/mL; age 64 [44-84] years), 733 lesions were identified (47% tumor-positive). Predictive abilities of both systems were comparable for all (AUC 76-78%) and CS cancers (AUCs 79%). The in-house system had higher overall and CS TDRs than PI-RADSv2 for categories 3 and 4 (P < 0.01 for both), with the greatest difference between the scoring systems seen in lesions scored category 4 (CS TDRs: in-house 65%, PI-RADSv2 22.1%). For lesions categorized as PI-RADSv2 = 4, characterization of suspicious/indeterminate extraprostatic extension (EPE) and equivocal findings across all mpMRI sequences contributed to significantly different TDRs for both systems (TDR range 19-75%, P < 0.05).
PI-RADSv2 behaves similarly to an existing validated system that relies on the number of sequences on which a lesion is seen. This prospective evaluation suggests that sequence positivity and suspicion of EPE can enhance PI-RADSv2 category 4 cancer detection.
1 Technical Efficacy: Stage 3 J. Magn. Reson. Imaging 2018;47:1326-1335.
前列腺影像报告和数据系统第 2 版(PI-RADSv2)为前列腺多参数磁共振成像(mpMRI)的解读提供了标准化的命名法。增加分类的额外特征可能有助于疾病分层。
前瞻性比较 PI-RADSv2 与用于检测 mpMRI 前列腺癌的定性内部系统。
前瞻性。
2015 年 5 月至 2016 年 5 月期间,共 338 例接受 mpMRI 的患者,随后进行 MRI/经直肠超声融合引导活检。
3T mpMRI(T W、扩散加权[DW]、表观扩散系数[ADC]图、b-2000 DWI 采集和动态对比增强[DCE] MRI)。
一名泌尿生殖系统放射科医生使用内部和 PI-RADSv2 5 类系统对 mpMRI 进行前瞻性阅读。
在基于病变的分析中,计算了所有 PI-RADSv2 和内部类别中的总体和临床显著(CS)肿瘤检测率(TDR)。通过受试者工作特征曲线(ROC)下面积(AUC)评估每个评分系统检测癌症的能力。在每个 PI-RADSv2 类别中,进一步根据其内部类别对病变进行分层,以确定是否可以通过合并两个系统的特征来提高 TDR。
在 338 例患者(中位前列腺特异性抗原[PSA]6.5[0.6-113.6]ng/ml;年龄 64[44-84]岁)中,共发现 733 个病变(47%肿瘤阳性)。两种系统对所有(AUC 76-78%)和 CS 癌症(AUCs 79%)的预测能力相当。对于类别 3 和 4,内部系统的总体和 CS TDR 均高于 PI-RADSv2(两者均 P<0.01),评分系统之间的最大差异见于评分类别 4 的病变(CS TDRs:内部系统 65%,PI-RADSv2 22.1%)。对于 PI-RADSv2=4 类病变,可疑/不确定的前列腺外延伸(EPE)和所有 mpMRI 序列的不确定发现的特征有助于两种系统的 TDR 显著不同(TDR 范围 19-75%,P<0.05)。
PI-RADSv2 的行为与依赖于病变在多少个序列上可见的现有经过验证的系统相似。这项前瞻性评估表明,序列阳性和 EPE 可疑性可以提高 PI-RADSv2 类别 4 癌症的检出率。
1 技术功效:第 3 阶段 J. Magn. Reson. Imaging 2018;47:1326-1335.