Lomax Anna J, Lim Jennifer, Cheng Robert, Sweeting Arianne, Lowe Patricia, McGill Neil, Shackel Nicholas, Chua Elizabeth L, McNeil Catriona
Chris O'Brien Lifehouse, Camperdown, NSW, Australia.
Concord Repatriation General Hospital, Sydney, NSW, Australia.
J Skin Cancer. 2018 Jan 21;2018:9602540. doi: 10.1155/2018/9602540. eCollection 2018.
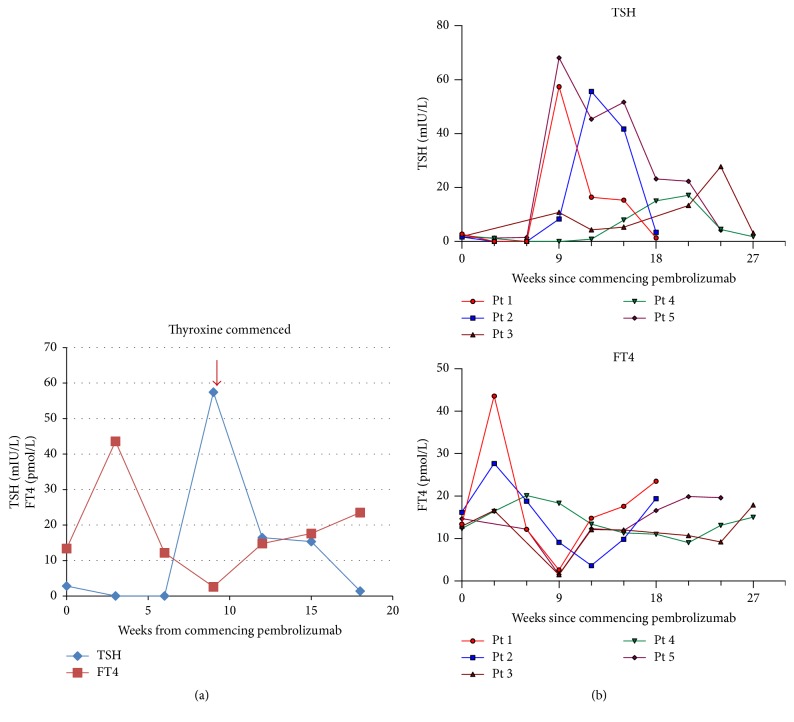
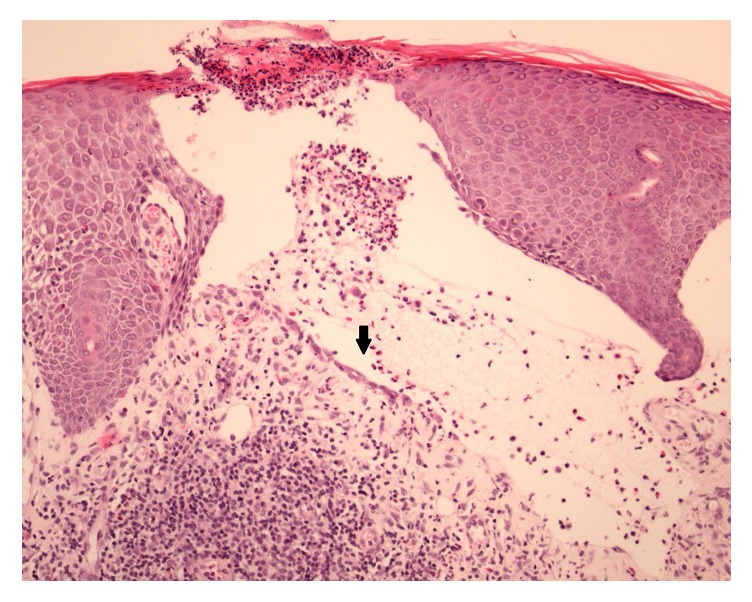
Immune checkpoint inhibitors (anti-PD-1 and anti-CTLA-4 antibodies) are a standard of care for advanced melanoma. Novel toxicities comprise immune-related adverse events (irAE). With increasing use, irAE require recognition, practical management strategies, and multidisciplinary care. We retrospectively evaluated the incidence, kinetics, and management of irAE in 41 patients receiving anti-PD-1 antibody therapy (pembrolizumab) for advanced melanoma. 63% received prior anti-CTLA-4 antibody therapy (ipilimumab). IrAE occurred in 54%, most commonly dermatological (24%), rheumatological (22%), and thyroid dysfunction (12%). Thyroiditis was characterised by a brief asymptomatic hyperthyroid phase followed by a symptomatic hypothyroid phase requiring thyroxine replacement. Transplant rejection doses of methylprednisolone were necessary to manage refractory hepatotoxicity. A bullous pemphigoid-like skin reaction with refractory pruritus responded to corticosteroids and neuropathic analgesia. Disabling grade 3-4 oligoarthritis required sulfasalazine therapy in combination with steroids. The median interval between the last dose of anti-CTLA-4 antibody and the first dose of anti-PD-1 therapy was 2.0 months (range: 0.4 to 22.4). Toxicities may occur late; this requires vigilance and multidisciplinary management which may allow effective anticancer therapy to continue. Management algorithms for thyroiditis, hypophysitis, arthralgia/arthritis, colitis, steroid-refractory hepatitis, and skin toxicity are discussed.
免疫检查点抑制剂(抗程序性死亡蛋白1和抗细胞毒性T淋巴细胞相关抗原4抗体)是晚期黑色素瘤的标准治疗方法。新出现的毒性反应包括免疫相关不良事件(irAE)。随着其使用的增加,irAE需要得到识别、切实可行的管理策略以及多学科护理。我们回顾性评估了41例接受抗程序性死亡蛋白1抗体治疗(帕博利珠单抗)的晚期黑色素瘤患者中irAE的发生率、发生情况及管理措施。63%的患者曾接受过抗细胞毒性T淋巴细胞相关抗原4抗体治疗(伊匹木单抗)。54%的患者出现了irAE,最常见的是皮肤病(24%)、风湿性疾病(22%)和甲状腺功能障碍(12%)。甲状腺炎的特点是有一个短暂的无症状甲状腺功能亢进期,随后是需要甲状腺素替代治疗的有症状甲状腺功能减退期。对于难治性肝毒性,需要使用大剂量甲基泼尼松龙进行治疗。一种伴有难治性瘙痒的大疱性类天疱疮样皮肤反应对皮质类固醇和神经性镇痛有反应。导致功能障碍的3 - 4级寡关节炎需要柳氮磺胺吡啶联合类固醇治疗。抗细胞毒性T淋巴细胞相关抗原4抗体的最后一剂与抗程序性死亡蛋白1治疗的第一剂之间的中位间隔时间为2.0个月(范围:0.4至22.4个月)。毒性反应可能会在后期出现;这需要保持警惕并进行多学科管理,从而使有效的抗癌治疗能够继续进行。文中讨论了甲状腺炎、垂体炎、关节痛/关节炎、结肠炎、类固醇难治性肝炎和皮肤毒性的管理算法。