Academic Urology Group, University of Cambridge, Addenbrooke's Hospital, Cambridge Biomedical Campus, Hills Road, Box 43, Cambridge, CB2 0QQ, UK.
Department of Urology, Addenbrooke's Hospital, Cambridge University Hospitals NHS Foundation Trust, Cambridge, CB2 0QQ, UK.
World J Urol. 2018 Sep;36(9):1341-1353. doi: 10.1007/s00345-018-2286-7. Epub 2018 Apr 2.
The widespread use of abdominal imaging has affected the epidemiology of renal cell carcinoma (RCC). Despite this, over 25% of individuals with RCC have evidence of metastases at presentation. Screening for RCC has the potential to downstage the disease.
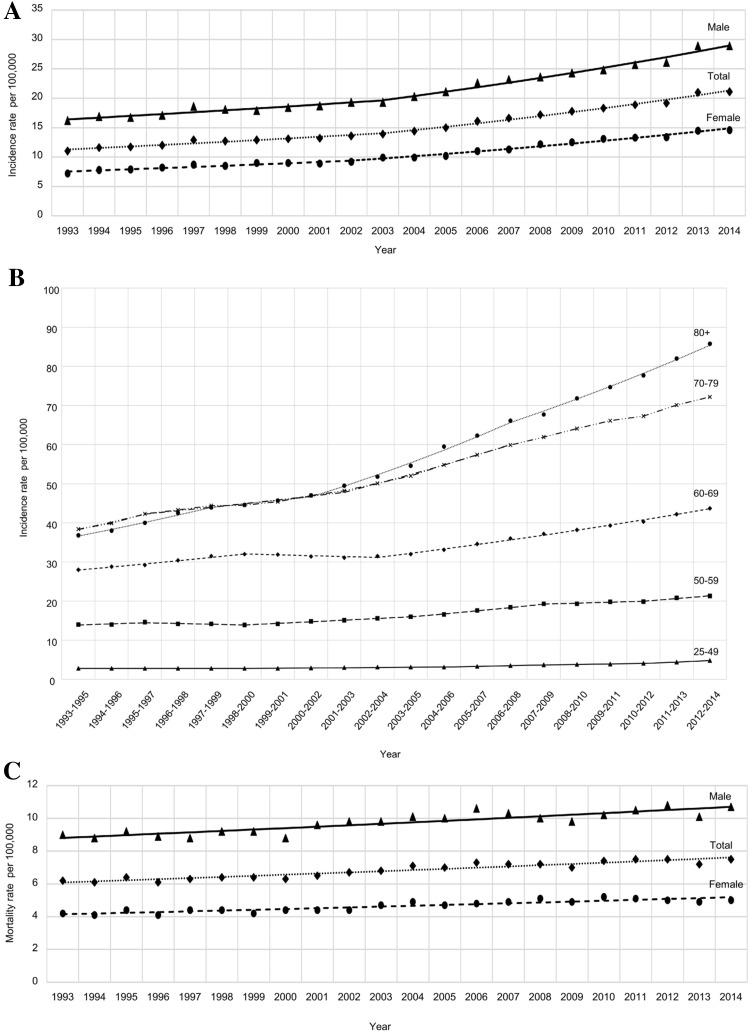
We performed a literature review on the epidemiology of RCC and evidence base regarding screening. Furthermore, contemporary RCC epidemiology data was obtained for the United Kingdom and trends in age-standardised rates of incidence and mortality were analysed by annual percentage change statistics and joinpoint regression.
The incidence of RCC in the UK increased by 3.1% annually from 1993 through 2014. Urinary dipstick is an inadequate screening tool due to low sensitivity and specificity. It is unlikely that CT would be recommended for population screening due to cost, radiation dose and increased potential for other incidental findings. Screening ultrasound has a sensitivity and specificity of 82-83% and 98-99%, respectively; however, accuracy is dependent on tumour size. No clinically validated urinary nor serum biomarkers have been identified. Major barriers to population screening include the relatively low prevalence of the disease, the potential for false positives and over-diagnosis of slow-growing RCCs. Individual patient risk-stratification based on a combination of risk factors may improve screening efficiency and minimise harms by identifying a group at high risk of RCC.
The incidence of RCC is increasing. The optimal screening modality and target population remain to be elucidated. An analysis of the benefits and harms of screening for patients and society is warranted.
腹部影像学的广泛应用影响了肾细胞癌(RCC)的流行病学。尽管如此,超过 25%的 RCC 患者在就诊时已有转移证据。RCC 的筛查有可能使疾病降期。
我们对 RCC 的流行病学和筛查证据进行了文献回顾。此外,还获得了英国当代 RCC 流行病学数据,并通过年度百分比变化统计和连接点回归分析发病率和死亡率的年龄标准化率的趋势。
1993 年至 2014 年期间,英国 RCC 的发病率每年增加 3.1%。尿沉渣检查因灵敏度和特异性低而不是一种合适的筛查工具。由于成本、辐射剂量和增加其他偶然发现的可能性,CT 不太可能被推荐用于人群筛查。筛查超声的灵敏度和特异性分别为 82-83%和 98-99%;然而,准确性取决于肿瘤大小。尚未发现经临床验证的尿液或血清生物标志物。人群筛查的主要障碍包括疾病的患病率相对较低、假阳性和对生长缓慢的 RCC 的过度诊断的潜在风险。基于危险因素组合的个体患者风险分层可能通过确定高危 RCC 患者群体来提高筛查效率并最大程度地减少危害。
RCC 的发病率正在增加。最佳的筛查方式和目标人群仍有待阐明。有必要对患者和社会的筛查获益和危害进行分析。