Hourani Siham, Motwani Kartik, Wajima Daisuke, Fazal Hanain, Jones Chad H, Doré Sylvain, Hosaka Koji, Hoh Brian L
Department of Neurosurgery, University of Florida, Gainesville, FL, United States.
Department of Anesthesiology, University of Florida, Gainesville, FL, United States.
Front Neurol. 2018 Mar 19;9:158. doi: 10.3389/fneur.2018.00158. eCollection 2018.
Local delivery of monocyte chemotactic protein-1 (MCP-1/CCL2) our drug-eluting coil has been shown to promote intrasaccular aneurysm healing an inflammatory pathway.
In this study, we validate the importance of local MCP-1 in murine aneurysm healing. Whether systemic, rather than local, delivery of MCP-1 can direct site-specific aneurysm healing has significant translational implications. If systemic MCP-1 is effective, then MCP-1 could be administered as a pill rather than by endovascular procedure. Furthermore, we confirm that MCP-1 is the primary effector in our MCP-1 eluting coil-mediated murine aneurysm healing model.
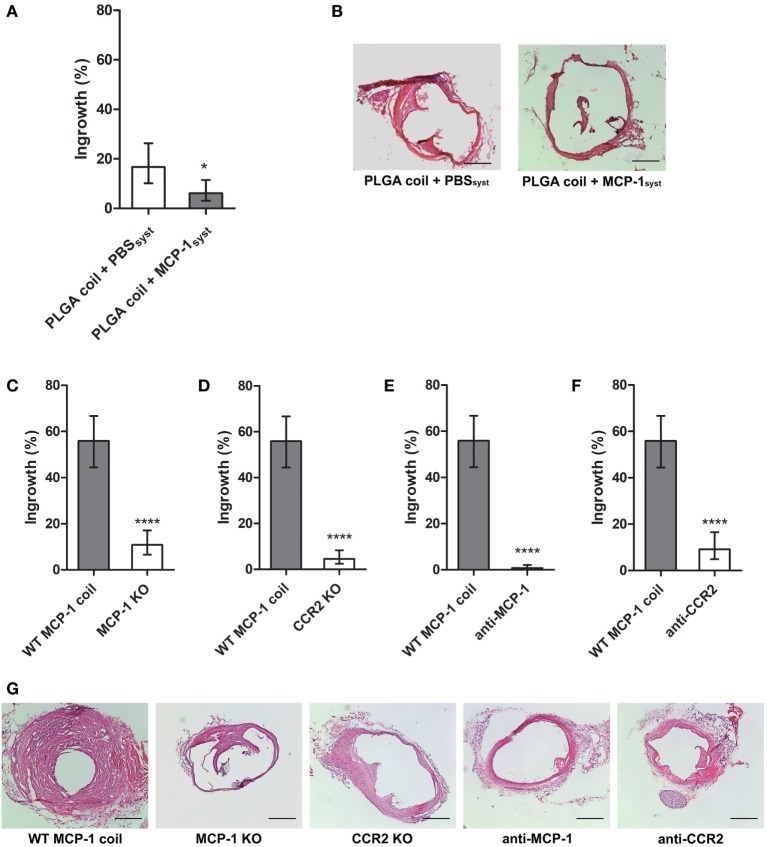
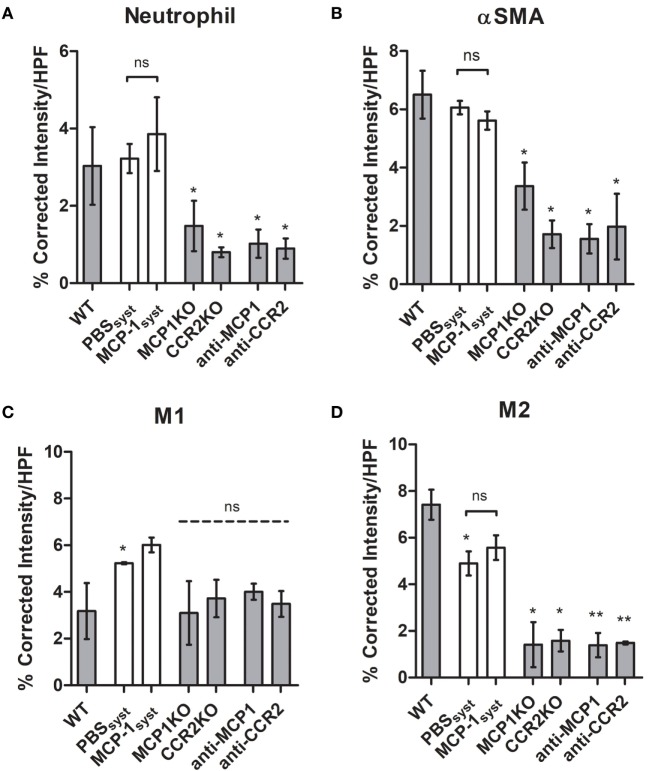
We compare aneurysm healing with repeated intraperitoneal MCP-1 versus vehicle injection, in animals with control poly(lactic-co-glycolic) acid (PLGA)-coated coils. We demonstrate elimination of the MCP-1-associated tissue-healing response by knockout of MCP-1 or CCR2 (MCP-1 receptor) and by selectively inhibiting MCP-1 or CCR2. Using immunofluorescent probing, we explore the cell populations found in healed aneurysm tissue following each intervention.
Systemically administered MCP-1 with PLGA coil control does not produce comparable aneurysm healing, as seen with MCP-1 eluting coils. MCP-1-directed aneurysm healing is eliminated by selective inhibition of MCP-1 or CCR2 and in MCP-1-deficient or CCR2-deficient mice. No difference was detected in M2 macrophage and myofibroblast/smooth muscle cell staining with systemic MCP-1 versus vehicle in aneurysm wall, but a significant increase in these cell types was observed with MCP-1 eluting coil implant and attenuated by MCP-1/CCR2 blockade or deficiency.
We show that systemic MCP-1 concurrent with PLGA-coated platinum coil implant is not sufficient to produce site-specific aneurysm healing. MCP-1 is a critical, not merely complementary, actor in the aneurysm healing pathway.
我们的药物洗脱微弹簧圈局部递送单核细胞趋化蛋白-1(MCP-1/CCL2)已被证明可促进囊内动脉瘤愈合,这是一条炎症途径。
在本研究中,我们验证局部MCP-1在小鼠动脉瘤愈合中的重要性。MCP-1的全身递送而非局部递送是否能指导位点特异性动脉瘤愈合具有重要的转化意义。如果全身应用MCP-1有效,那么MCP-1可以制成药丸给药,而不必通过血管内手术给药。此外,我们证实MCP-1是我们的MCP-1洗脱微弹簧圈介导的小鼠动脉瘤愈合模型中的主要效应因子。
我们在植入对照聚乳酸-乙醇酸共聚物(PLGA)包被微弹簧圈的动物中,比较重复腹腔注射MCP-1与注射赋形剂后的动脉瘤愈合情况。我们通过敲除MCP-1或CCR2(MCP-1受体)以及选择性抑制MCP-1或CCR2,证明消除了与MCP-1相关的组织愈合反应。使用免疫荧光探针,我们探究了每种干预后愈合的动脉瘤组织中的细胞群。
与MCP-1洗脱微弹簧圈相比,全身给予MCP-1并联合PLGA包被微弹簧圈对照不能产生类似的动脉瘤愈合效果。通过选择性抑制MCP-1或CCR2以及在MCP-1缺陷或CCR2缺陷小鼠中,MCP-1介导的动脉瘤愈合被消除。在动脉瘤壁中,全身应用MCP-1与应用赋形剂相比,M2巨噬细胞和成肌纤维细胞/平滑肌细胞染色未检测到差异,但在植入MCP-1洗脱微弹簧圈后这些细胞类型显著增加,并且通过MCP-1/CCR2阻断或缺陷而减弱。
我们表明,全身应用MCP-1并同时植入PLGA包被的铂微弹簧圈不足以产生位点特异性动脉瘤愈合。MCP-1是动脉瘤愈合途径中的关键因素,而不仅仅是辅助因素。