Department of BMT, Great Ormond Street Hospital for Children, National Health Service (NHS) Foundation Trust, London, United Kingdom.
Department of Adolescent BMT, University College Hospital, NHS Foundation Trust, London, United Kingdom.
Blood Adv. 2018 Apr 10;2(7):777-786. doi: 10.1182/bloodadvances.2017014449.
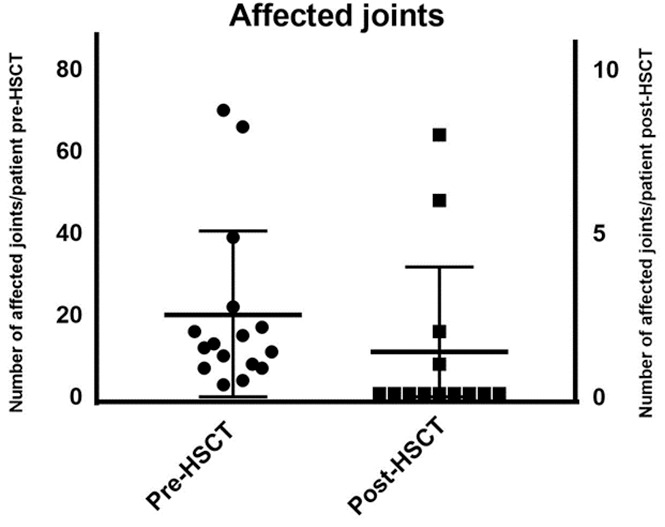
Patients with juvenile idiopathic arthritis (JIA) can experience a severe disease course, with progressive destructive polyarthritis refractory to conventional therapy with disease-modifying antirheumatic drugs including biologics, as well as life-threatening complications including macrophage activation syndrome (MAS). Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is a potentially curative immunomodulatory strategy for patients with such refractory disease. We treated 16 patients in 5 transplant centers between 2007 and 2016: 11 children with systemic JIA and 5 with rheumatoid factor-negative polyarticular JIA; all were either refractory to standard therapy, had developed secondary hemophagocytic lymphohistiocytosis/MAS poorly responsive to treatment, or had failed autologous HSCT. All children received reduced toxicity fludarabine-based conditioning regimens and serotherapy with alemtuzumab. Fourteen of 16 patients are alive with a median follow-up of 29 months (range, 2.8-96 months). All patients had hematological recovery. Three patients had grade II-IV acute graft-versus-host disease. The incidence of viral infections after HSCT was high, likely due to the use of alemtuzumab in already heavily immunosuppressed patients. All patients had significant improvement of arthritis, resolution of MAS, and improved quality of life early following allo-HSCT; most importantly, 11 children achieved complete drug-free remission at the last follow-up. Allo-HSCT using alemtuzumab and reduced toxicity conditioning is a promising therapeutic option for patients with JIA refractory to conventional therapy and/or complicated by MAS. Long-term follow-up is required to ascertain whether disease control following HSCT continues indefinitely.
患有幼年特发性关节炎(JIA)的患者可能会经历严重的疾病过程,表现为常规治疗(包括生物制剂)无效的进行性破坏性多发性关节炎,以及包括巨噬细胞活化综合征(MAS)在内的危及生命的并发症。异基因造血干细胞移植(allo-HSCT)是一种针对此类难治性疾病的潜在治愈性免疫调节策略。我们在 2007 年至 2016 年间在 5 个移植中心治疗了 16 名患者:11 名儿童患有全身型 JIA,5 名患有类风湿因子阴性多关节型 JIA;所有患者均对标准治疗无效,或已发展为继发性噬血细胞性淋巴组织细胞增多症/MAS(对治疗反应不佳),或自体 HSCT 失败。所有儿童均接受了减少毒性的氟达拉滨为基础的预处理方案和用阿仑单抗进行血清治疗。16 名患者中有 14 名存活,中位随访时间为 29 个月(范围,2.8-96 个月)。所有患者均有血液学恢复。3 名患者发生 2-4 级急性移植物抗宿主病。HSCT 后病毒感染的发生率很高,可能是由于在已经严重免疫抑制的患者中使用了阿仑单抗。所有患者在 allo-HSCT 后早期关节炎均显著改善,MAS 得到缓解,生活质量提高;最重要的是,11 名儿童在最后一次随访时达到了无药物完全缓解。对于常规治疗无效且并发 MAS 的 JIA 患者,使用阿仑单抗和减少毒性预处理的 allo-HSCT 是一种有前途的治疗选择。需要长期随访以确定 HSCT 后疾病控制是否持续无限期。